Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
On Jan 17, 2022, Nature Reviews Clinical Oncology (IF: 66.675) published a review entitled "Harnessing cytokines and chemokines for cancer therapy" [1]. In this article, the authors conclude the high potential of targeting chemokine receptors in tumor. Intriguingly, the report revealed that CCR4 as a key tumor-associated chemokine receptor, CCR4 antagonist could significantly reduce Treg cells accumulation in the tumor and improve Treg cell-induced tumor immunosuppression [1]. CCR4 as an attractive therapeutic target, there existed one FDA approval CCR4 antagonist for hematologic T-cell lymphoma treatment. Beyond this, several studies in recent years have shown that CCR4 also play key roles in different solid tumors. Thereby, what does CCR4 do? How is CCR4 receptor involved in immune response to tumor cells? Here's a brief overview of CCR4 and its possible clinical applications in tumor and other diseases.
3. How's the Mechanisms of CCR4-Mediated Signaling Pathway?
What does CCR4 stand for? CCR4 stands for C-C chemokine receptor type 4 (CCR4), also known as CD194, which belongs to the G protein-coupled receptor family. CCR4 consists of a polypeptide chain with a 7subtransmembrane structural domain. It contains 360 amino acids with a 41kD molecular weight. What cells express CCR4? CCR4 is mainly expressed in various lymphocytes and tissues. There are various chemokines identified as CCR4 ligands [2]. As an important chemokine receptor, CCR4 binds to the chemokine ligands and performs its function in human autoimmune diseases, such as atopic dermatitis (AD), asthma, and cutaneous T-cell lymphoma (CTCL) [3]. Indeed, it was originally noted that chemokines were important in the inflammatory response. At present, accumulated research suggested that chemokines in combination with their receptors play a key role in the tumor cells infiltration, distant metastasis, and other biological behaviors. CCR4 as a key chemokine receptor in tumor metastasis, several studies have demonstrated that high CCR4 expression is closely associated with poor prognosis in hematological and solid tumors. Collectively, CCR4 is expected to be a new therapeutic target for cancer immunotherapy.
The identified CCR4 ligands are CCL17, CCL22, RANTES, MCP-1, MIP-1α, and the newest ligand CKLF1 [1-3, 5]. Current studies have focused on the interaction between CCR4 and the high-affinity ligands CCL17 and CCL22. CCL17, also known as thymic activation regulatory chemokine (TARC), is expressed mainly in the thymus and other tissues such as lung, colon, and small intestine. CCL22 often named macrophage-derived chemokine (MDC), is mainly produced by dendritic cells and macrophages, which plays an important role in regulating the differentiation and proliferation of T lymphocytes, B lymphocytes, and dendritic cells by binding to the cell surface receptor CCR4. Beyond this, CCL17 and CCL22, as high-affinity receptors for CCR4, many findings have shown that the ligands with CCR4 receptor play an essential part in the development of inflammatory diseases and various tumors [6].
CCL17 and CCL22, the most common ligands of CCR4, have been increasingly studied to show their role in the immune response, especially in tumor cells. However, the roles that chemokines and their receptors in tumor development and progression are complex and the mechanisms of how they activate certain signal transduction pathways have not been fully understood.
Current studies suggested that CCR4 combined with CCL17/CCL22 induces an enrichment of Treg cells in the tumor microenvironment. Treg as a type of T cell can suppress the function of immune effector cells through a variety of mechanisms. To some extent, Treg cells are key factors in tumor immune escape, which can effectively avoid the autoimmune response. Thus, it is these Treg cells that are used by tumor cells to cause immune escape (click to learn more about Treg cells). As presented in the Figure 1, CCR4 exerts immune effects through CCR4+Treg cells and is involved in the invasion and metastasis of different tumor cells, lymphangiogenesis and lymphocyte presentation, production of tumor inflammatory mediators, etc [7]. Specifically, CCR4 on the surface of Treg cells binding to its chemokine ligands, caused robust Treg accumulation and thus promoting tumor immune evasion, with a similar mechanism of Treg cell-specific target CCR8 (click for CCR8 related article).
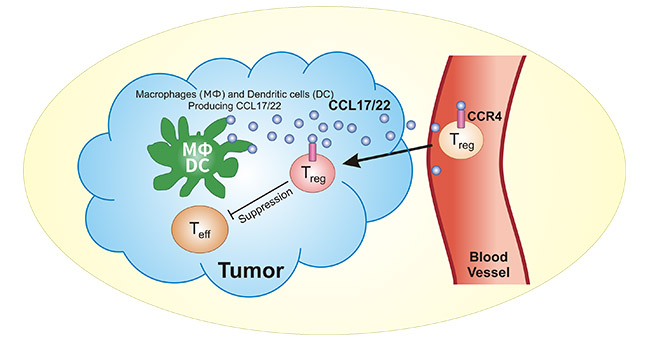
Figure1. CCR4 on Treg cells binds to CCL17/CCL22 induces tumor immunosuppression
CCR4 as newly recognized chemokine receptor, a growing number of studies suggested that CCR4 binding to the chemokines CCL17/CCL22 is involved in many important physiological and pathological effects in vivo, which is associated with allergic inflammatory diseases (atopic dermatitis), autoimmune diseases (rheumatoid arthritis), and many tumors (T-cell lymphoma, breast cancer, lung cancer, gastric cancer, and others) [8].
Lately, a breakthrough in Allergic Dermatitis (AD) treatment has been achieved with a CCR4 inhibitor, RPT193. The results indicated that patients were well tolerated and safe in clinical studies, especially in patients with severe AD. The report further adds that RPT193 treatment is superior to IL-4R antibody therapy. It plays a crucial role in AD and asthma either by blocking the CCR4 receptor expression on Th2 cells, or partly inhibiting the migration of Th2 cells to inflammatory tissues [9]. The findings implied the high potential of RPT193 as well as CCR4-targeted therapy in allergic inflammatory diseases.
Additionally, chemokine receptor CCR4 expression on Treg cells is significantly increased in the peripheral blood of patients with Rheumatoid Arthritis (RA) and Systemic Lupus Erythematosus (SLE), of which abnormal CCR4 expression correlates with disease progression. It could be concluded that CCR4 receptor on Tregs cells induces the migration ability, which further manipulates Treg cell activity and contributes to the immunosuppressive [10]. Therefore, it is necessary to deeply understand the relationship between Treg cell and CCR4 expression, which might provide alternative strategies for the RA and SLE treatment.
Importantly, the crucial role of CCR4 in tumors has also been amply demonstrated in recent years. The previous studies mainly focus on CCR4 and hematologic tumors such as adult T-cell leukemia/lymphoma [11]. Currently, studies have demonstrated that CCR4 expression is partly responsible for various malignancies such as breast cancer [12], lung cancer [13], gastric cancer [14], pancreatic cancer [15], liver cancer [16], and colorectal cancer [17].
In hematopoietic or other malignancies, CCR4 often binding to corresponding ligands induce immune escape. For example, in patients with T-cell leukemia, CCL17 and CCL22 secreted by tumor cells create a microenvironment for tumor immune escape, which contributes to the chemotactic aggregation of CCR4+ Treg cells [11]. Similarly, in breast cancer, CCR4/CCL22 induces Treg cells to migrate into the lymphoid infiltrating tissue in tumor, promoting Treg cell expression and tumor growth [12]. Abnormal Treg cell accumulation is closely related to a poorer prognosis for tumor patients. Namely, CCR4 on Treg cells binding to the ligands CCL17 and CCL22 promote the chemotactic behavior of Treg cell, which induce the immune escape in tumors. Taken together, CCR4, as a surface marker of Treg cells, appears to be promising target in cancer immunotherapy.
Apparently, CCR4 as the important chemokine receptor on Treg cells, is providing new insights for clinical research in tumors or other diseases. It should be noted that first CCR4 antagonist (Mogamulizumab) by RAPT Therapeutics company was approved by the FDA in 2018, which specifically treat mycosis fungoides (MF) or Sézary syndrome (SS). Significantly, the company is developing another two CCR4 drug candidates, FLX475 for tumor and RPT193 for atopic dermatitis. Data from the Therapeutic Antibody Database indicated that there are several CCR4 antibodies in the preclinical phase, but no specific clinical information has been published. Although the CRR4 is still at its early stages of clinical use and require much more investigations to its applications, the key roles of CCR4 + Tregs in tumor immunosuppression received increasing attention. Many findings indicated that CCR4 might serve as a new target in tumors as well allergic or autoimmune diseases.
To fully serve the pharmaceutical companies in their research on CCR4 in allergic diseases, autoimmune diseases, and especially in tumors, CUSABIO offers CCR4 active protein products (Code: CSB-MP004843HU; Code: CSB-CF004843HU) to help you in your research on the CCR4 mechanism or its possible clinical applications.
● Recombinant Human C-C chemokine receptor type 4 (CCR4)-VLPs (Active)
CSB-MP004843HU is detected by Mouse anti-6*His monoclonal antibody.
Immobilized Human CCR4 at 10 μg/ml can bind Anti-CCR4 recombinant antibody (CSB-RA004843MA01HU), the EC 50 is 362.3-630.8 ng/mL.
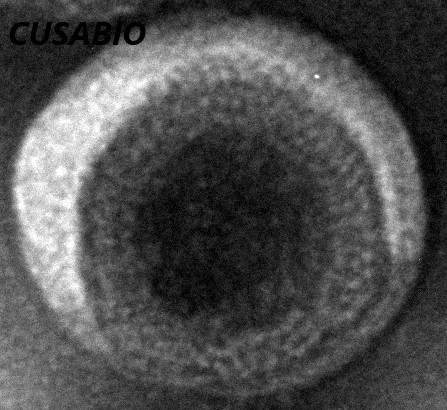
The presence of VLP-like structures was confirmed by TEM.
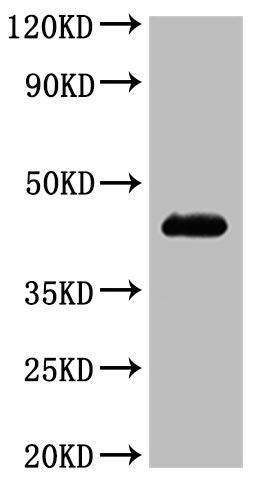
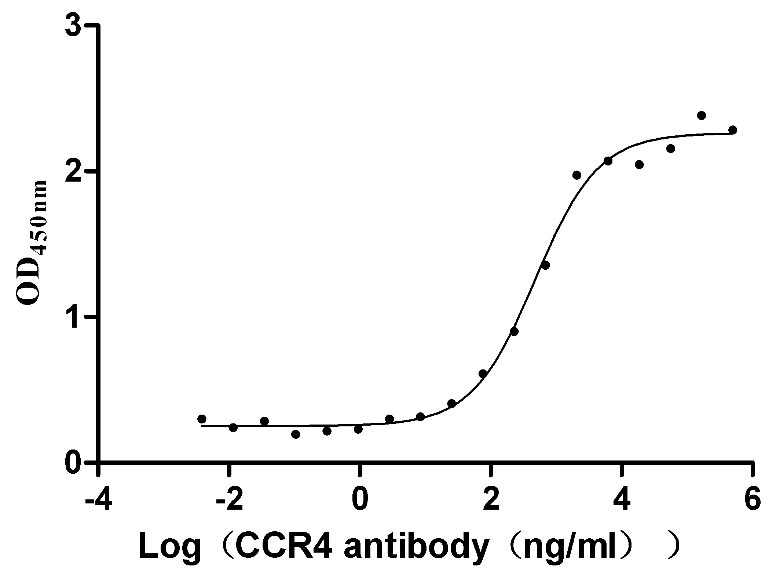
● Recombinant Human C-C chemokine receptor type 4 (CCR4) (Active)
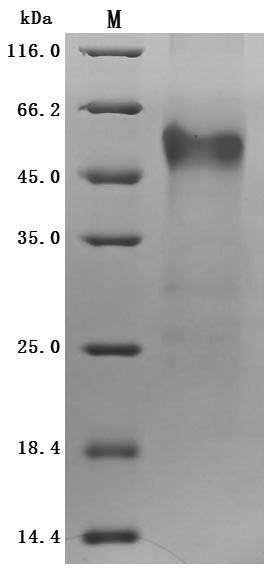
Purity was greater than 85% as determined by SDS-PAGE. (Tris-Glycine gel) Discontinuous SDS-PAGE (reduced) with 5% enrichment gel and 15% separation gel.
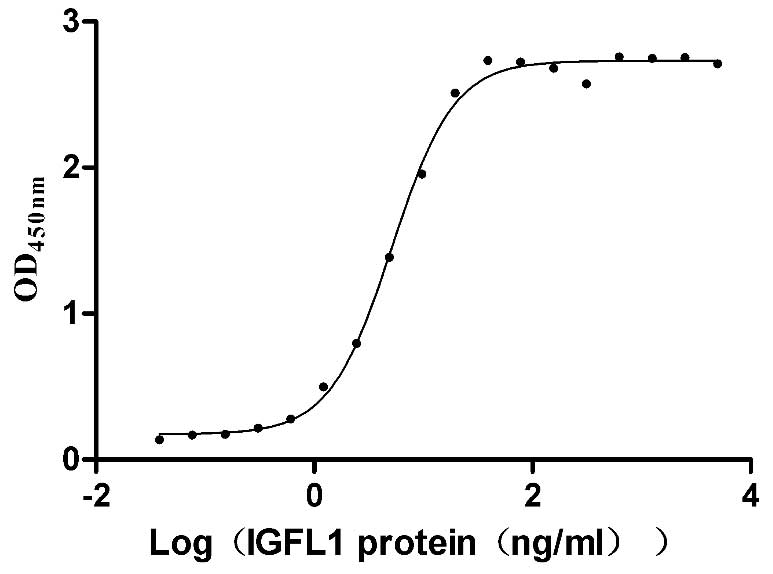
CCR4 at 5 μg/ml can bind Anti-CCR4 recombinant antibody (CSB-RA004843MA01HU), the EC 50is 7.818-21.25 ng/mL.
References
[1] Propper, David J., and Frances R. Balkwill. "Harnessing cytokines and chemokines for cancer therapy." Nature Reviews Clinical Oncology (2022): 1-17.
[2] Fujii, Keiichiro, et al. "Immunohistochemistry for CCR4 C‐terminus predicts CCR4 mutations and mogamulizumab efficacy in adult T‐cell leukemia/lymphoma." The Journal of Pathology: Clinical Research 7.1 (2021): 52-60.
[3] Yoshie, Osamu, and Kouji Matsushima. "CCR4 and its ligands: from bench to bedside." International immunology 27.1 (2015): 11-20.
[4] Oliveira, S. H. P., and N. W. Lukacs. "The role of chemokines and chemokine receptors in eosinophil activation during inflammatory allergic reactions." Brazilian Journal of Medical and Biological Research 36.11 (2003): 1455-1463.
[5] Ai, Q. D., et al. "IMM-H004 therapy for permanent focal ischemic cerebral injury via CKLF1/CCR4-mediated NLRP3 inflammasome activation." Translational Research 212 (2019): 36-53.
[6] Kumai, Takumi, et al. "CCL17 and CCL22/CCR4 signaling is a strong candidate for novel targeted therapy against nasal natural killer/T-cell lymphoma." Cancer Immunology, Immunotherapy 64.6 (2015): 697-705.
[7] Ketcham, John M., Lisa A. Marshall, and Oezcan Talay. "CCR4 antagonists inhibit Treg trafficking into the tumor microenvironment." ACS Medicinal Chemistry Letters 9.10 (2018): 953-955.
[8] Solari, Roberto, and James E. Pease. "Targeting chemokine receptors in disease–a case study of CCR4." European Journal of Pharmacology 763 (2015): 169-177.
[9] Cheng, Laurence, et al. "Development and first-in-human characterization of a potent oral CCR4 antagonist for the treatment of atopic dermatitis." Journal of Investigative Dermatology. Vol. 140. No. 7. STE 800, 230 PARK AVE, NEW YORK, NY 10169 USA: ELSEVIER SCIENCE INC, 2020.
[10] Flytlie, Helene Aarslev, et al. "Expression of MDC/CCL22 and its receptor CCR4 in rheumatoid arthritis, psoriatic arthritis and osteoarthritis." Cytokine 49.1 (2010): 24-29.
[11] Ishida, Takashi, et al. "Clinical significance of CCR4 expression in adult T-cell leukemia/lymphoma: its close association with skin involvement and unfavorable outcome." Clinical Cancer Research 9.10 (2003): 3625-3634.
[12] Olkhanud, Purevdorj B., et al. "Breast cancer lung metastasis requires expression of chemokine receptor CCR4 and regulatory T cells." Cancer research 69.14 (2009): 5996-6004.
[13] Kurose, Koji, et al. "Increase in activated Treg in TIL in lung cancer and in vitro depletion of Treg by ADCC using an antihuman CCR4 mAb (KM2760)." Journal of Thoracic Oncology 10.1 (2015): 74-83.
[14] Lee, Jun Ho, et al. "The chemokine receptor CCR4 is expressed and associated with a poor prognosis in patients with gastric cancer." Annals of surgery 249.6 (2009): 933-941.
[15] Moritz, Rapp, et al. "ITOC2–025. Transduction with CC-chemokine receptor type 4 (CCR4) enhances tumour-specific migration of adoptively transferred T cells in a model of pancreatic cancer." European Journal of Cancer 51 (2015): S9.
[16] Takahashi, Akinori, et al. "The CCR4–NOT complex maintains liver homeostasis through mRNA deadenylation." Life science alliance 3.5 (2020).
[17] Ou, Baochi, et al. "CCR4 promotes metastasis via ERK/NF-κB/MMP13 pathway and acts downstream of TNF-α in colorectal cancer." Oncotarget 7.30 (2016): 47637.


Comments
Leave a Comment