Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
| Code | CSB-EP871385HU |
| Abbreviation | Recombinant Human KAAG1 protein (Active) |
| MSDS | |
| Size | $9.9 |
| Promotion |

|
| Order now | |
| Image |
|
| Have Questions? | Leave a Message or Start an on-line Chat |
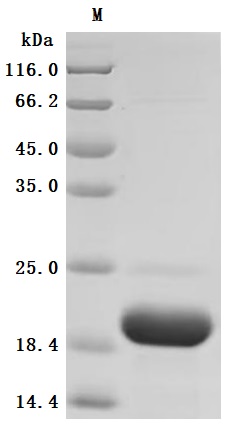
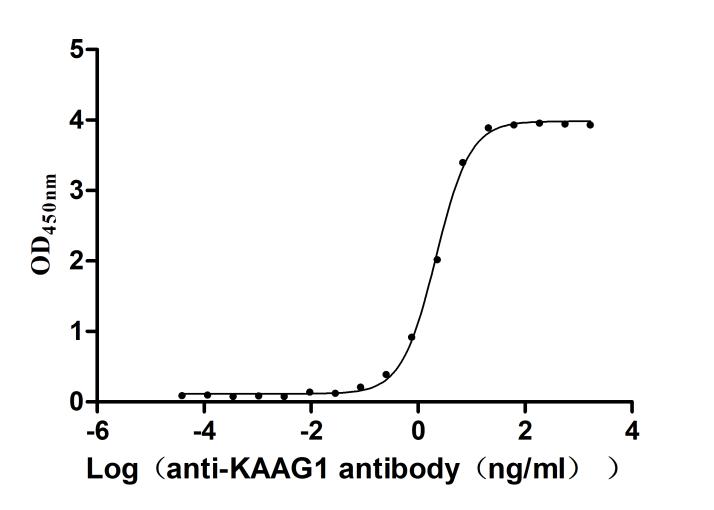
The recombinant human KAAG1 Protein is a highly purified biological reagent expressed in Escherichia coli, comprising amino acid residues 1-84 of the full-length human KAAG1 sequence with a C-terminal 6xHis tag for efficient purification. Produced as a lyophilized powder, this recombinant KAAG1 protein demonstrates exceptional quality control parameters, exhibiting >90% purity as verified by SDS-PAGE analysis and containing <1.0 endotoxin units per microgram (EU/μg) when assessed through the LAL method. Functional characterization via ELISA reveals its strong binding capability to the anti-KAAG1 recombinant antibody (CSB-RA871385MA1HU), with an effective concentration for half-maximal response (EC50) ranging between 2.040 and 2.284 ng/mL when immobilized at 2 μg/mL. These biochemical and functional properties establish this engineered protein as a reliable tool for studying KAAG1-mediated biological processes, particularly in antibody interaction analyses and molecular binding assays requiring precise quantitation of protein- ligand interactions.
Human KAAG1 is a protein involved in various kidney-related conditions and physiological processes. As a protein expressed in normal kidneys, KAAG1 likely plays a role in cellular processes associated with kidney health, and it becomes particularly relevant in pathological situations such as acute kidney injury and glomerulonephritis.
KAAG1 has been linked to the immunogenicity observed in kidney transplantation contexts. Studies indicate that specific antigens, including KAAG1, can be recognized by antibodies in the serum of transplant recipients, potentially influencing graft rejection rates [1][2]. This relationship highlights the role of KAAG1 not only as a marker of renal tissue but also as part of the immunological environment surrounding kidney transplantation, where its expression can contribute to humoral immune responses critical in graft acceptance or rejection.
Moreover, the significance of KAAG1 extends into the realm of kidney disease, particularly regarding hepatitis B virus (HBV)-associated nephropathy. Research indicates that HBV infection can lead to kidney damage manifesting as glomerulonephritis, wherein KAAG1 may serve as an immunological target, possibly influencing the pathological mechanisms underlying HBV's effects on kidney structures [3][4].
The interaction of KAAG1 with various cellular processes adds complexity to its functional profile. Studies on acute kidney injury suggest that different signaling pathways may intersect with KAAG1 activity [5]. For instance, the epithelial cell response to injury is crucial, where KAAG1 may influence repair mechanisms or cell proliferation, indicating its potential integral role in both renal tissue integrity and the reparative process following injury.
Furthermore, understanding KAAG1's role in renal fibrosis and inflammation is essential, particularly as macrophage-derived microvesicles interplay with antigens like KAAG1 during renal inflammation, potentially modulating the disease state and influencing therapeutic approaches [6][7].
References:
[1] L. Li, T. Sigdel, M. Vitalone, S. Lee, & M. Sarwal. Differential immunogenicity and clinical relevance of kidney compartment specific antigens after renal transplantation. Journal of Proteome Research, vol. 9, no. 12, p. 6715-6721, 2010. https://doi.org/10.1021/pr1008674
[2] R. Dinavahi, A. George, et al. Antibodies reactive to non-hla antigens in transplant glomerulopathy. Journal of the American Society of Nephrology, vol. 22, no. 6, p. 1168-1178, 2011. https://doi.org/10.1681/asn.2010111183
[3] J. Zhang, X. Zhang, Y. Sun, B. Long, X. Wang, & X. Li. Reactivation of resolved hepatitis b virus infection combined with nephrotic syndrome in a patient after allogeneic haematopoietic stem cell transplantation. BMC Infectious Diseases, vol. 19, no. 1, 2019. https://doi.org/10.1186/s12879-019-3690-3
[4] T. Peng, T. Xie, L. Liu, J. Zhen, & X. Yang. Analysis of clinical features and pathology of serum hbsag positive glomerulonephritis. Journal of Medical Virology, vol. 90, no. 3, p. 612-615, 2017. https://doi.org/10.1002/jmv.24959
[5] J. Cao, B. Wang, et al. Exosomal mir-125b-5p deriving from mesenchymal stem cells promotes tubular repair by suppression of p53 in ischemic acute kidney injury. Theranostics, vol. 11, no. 11, p. 5248-5266, 2021. https://doi.org/10.7150/thno.54550
[6] A. Jackson, M. Kuperman, & R. Montgomery. Multiple hyperacute rejections in the absence of detectable complement activation in a patient with endothelial cell reactive antibody. American Journal of Transplantation, vol. 12, no. 6, p. 1643-1649, 2012. https://doi.org/10.1111/j.1600-6143.2011.03955.x
[7] T. Tang, L. Lv, et al. Employing macrophage-derived microvesicle for kidney-targeted delivery of dexamethasone: an efficient therapeutic strategy against renal inflammation and fibrosis. Theranostics, vol. 9, no. 16, p. 4740-4755, 2019. https://doi.org/10.7150/thno.33520
There are currently no reviews for this product.

