Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
| Code | CSB-RA548583A0HU |
| Size | US$210 |
| Order now | |
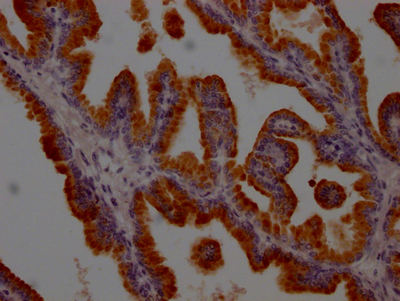
| Image |
|
| Have Questions? | Leave a Message or Start an on-line Chat |
| Application | Recommended Dilution |
|---|---|
| IHC | 1:50-1:200 |
The KLK3 recombinant monoclonal antibody is prepared using protein and DNA recombinant technology. Initially, mice were immunized with a synthesized peptide from human KLK3. After a certain time, the spleen of mice was isolated under aseptic conditions, and the total RNA of spleen cells was extracted. The cDNA synthesized by RNA reverse transcription was used as a template for PCR amplification of the KLK3 antibody gene. The KLK3 antibody gene was then introduced into a vector and transfected into host cells for culture. The KLK3 recombinant monoclonal antibody was purified from the supernatant of cell culture by affinity chromatography and can be used to detect human KLK3 protein in ELISA and IHC experiments.
The KLK3 protein, also known as the prostate-specific antigen (PSA), is a serine protease primarily produced by the prostate gland in men. Its main function is to cleave semenogelins, which are proteins that contribute to the gel-like texture of semen, allowing the semen to liquefy and release sperm for fertilization. In addition to its role in semen liquefaction, KLK3 has been implicated in other biological processes, including regulation of cell growth, apoptosis, and angiogenesis.
There are currently no reviews for this product.

