Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
| Code | CSB-MP004844HU |
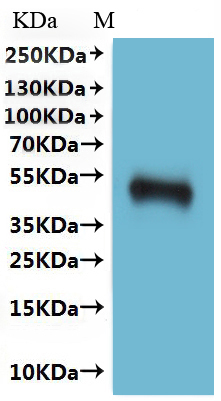
| Abbreviation | Recombinant Human CCR5 protein-VLPs (Active) |
| MSDS | |
| Size | $558 |
| Order now | |
| Image |
|
| Have Questions? | Leave a Message or Start an on-line Chat |
The recombinant human CCR5 protein is produced through virus-like particles (VLPs) technology. The CCR5 gene segment encoding amino acids 1-352 of the human CCR5 protein is cloned into a lentiviral vector incorporating a C-terminal 10xHis-tag. HEK293 cells are transfected with the recombinant lentiviral vector, and a selective antibiotic is added to identify successfully transfected cells. After successfully expressing the CCR5 protein, the cells are transfected with the viral capsid proteins required to express VLPs, which self-assemble into VLPs in the cells. When the cell culture reaches a certain density and expresses enough VLPs, the cells are lysed by ultrasonic treatment or chemical reagents to release the VLPs, which are separated through sucrose or other density gradient-mediated ultracentrifugation. The recombinant CCR5 proteins (VLPs) are further purified through affinity chromatography from the supernatant.
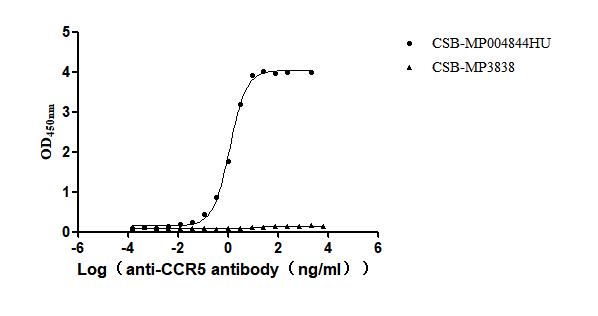
Their endotoxin levels are less than 1.0 EU/μg as measured by the LAL method. Functional ELISA confirms this recombinant CCR5 protein binds the CCR5 recombinant antibody (CSB-RA004844MA1HU), with an EC50 between 1.099 and 1.287 ng/mL.
Human CCR5 is a crucial chemokine receptor that plays a significant role in the immune system and is notably recognized for its involvement as a co-receptor for the entry of HIV-1 into host cells. CCR5 mainly mediates the migration of immune cells to sites of inflammation by binding to its ligands, such as CCL5 (RANTES), CCL3 (MIP-1α), and CCL4 (MIP-1β) [3][4]. This receptor is predominantly expressed on T cells, macrophages, and dendritic cells, which are essential components of the immune response [3]. The interaction between CCR5 and HIV-1 is particularly significant; the virus utilizes CCR5, along with CD4, to gain entry into host cells, which is a critical step in the pathogenesis of HIV infection [5].
Research has shown that variations in CCR5 expression can influence immune responses and disease susceptibility. The CCR5Δ32 mutation results in a nonfunctional receptor that is unable to reach the cell surface, providing homozygous individuals with a high level of resistance to HIV infection [1][2]. Individuals with the CCR5Δ32 allele exhibit altered immune responses, which can lead to increased susceptibility to certain infections, such as influenza [6][7]. Additionally, CCR5 has been implicated in cancer, where its expression levels can affect tumor progression and metastasis [8][9]. Studies have demonstrated that CCR5 antagonists, such as maraviroc, can inhibit the proliferation of cancer cells and modulate immune responses, highlighting the receptor's multifaceted role in both infectious diseases and cancer [3][9].
Furthermore, CCR5's involvement extends to autoimmune diseases, where polymorphisms in the CCR5 gene have been associated with conditions like systemic lupus erythematosus and rheumatoid arthritis [10][11]. The receptor's signaling pathways are critical for T cell activation and cytokine production [12]. Thus, CCR5 is a vital component in the immune system and the pathology of various diseases, making it a significant target for therapeutic interventions.
References:
[1] J. Ellwanger, B. Kulmann-Leal, V. Kaminski, A. Rodrigues, & M. Bragatte. Beyond hiv infection: neglected and varied impacts of ccr5 and ccr5δ32 on viral diseases, Virus Research, vol. 286, p. 198040, 2020. https://doi.org/10.1016/j.virusres.2020.198040
[2] P. Spagnolo, E. Renzoni, A. Wells, S. Copley, S. Desai, H. Sato, et al. C-c chemokine receptor 5 gene variants in relation to lung disease in sarcoidosis, American Journal of Respiratory and Critical Care Medicine, vol. 172, no. 6, p. 721-728, 2005. https://doi.org/10.1164/rccm.200412-1707oc
[3] S. Woollard and G. Kanmogne. Maraviroc: a review of its use in hiv infection and beyond, Drug Design Development and Therapy, p. 5447, 2015. https://doi.org/10.2147/dddt.s90580
[4] A. Amara, A. Vidy, G. Boulla, K. Mollier, J. García-Pérez, J. Alcamí, et al. G protein-dependent ccr5 signaling is not required for efficient infection of primary t lymphocytes and macrophages by r5 human immunodeficiency virus type 1 isolates, Journal of Virology, vol. 77, no. 4, p. 2550-2558, 2003. https://doi.org/10.1128/jvi.77.4.2550-2558.2003
[5] J. Nahabedian, A. Sharma, M. Kaczmarek, G. Wilkerson, S. Sawyer, & J. Overbaugh. Owl monkey ccr5 reveals synergism between cd4 and ccr5 in hiv-1 entry, Virology, vol. 512, p. 180-186, 2017. https://doi.org/10.1016/j.virol.2017.09.018
[6] F. Tsamis, S. Gavrilov, F. Kajumo, C. Seibert, S. Kuhmann, T. Ketas, et al. Analysis of the mechanism by which the small-molecule ccr5 antagonists sch-351125 and sch-350581 inhibit human immunodeficiency virus type 1 entry, Journal of Virology, vol. 77, no. 9, p. 5201-5208, 2003. https://doi.org/10.1128/jvi.77.9.5201-5208.2003
[7] A. Martín-Leal, R. Blanco, J. Casas, M. Sáez, E. Rodríguez-Bovolenta, I. Rojas, et al. ccr5 deficiency impairs cd4+ t‐cell memory responses and antigenic sensitivity through increased ceramide synthesis, The Embo Journal, vol. 39, no. 15, 2020. https://doi.org/10.15252/embj.2020104749
[8] M. Rossol, M. Pierer, S. Arnold, G. Keyßer, H. Burkhardt, C. Baerwald, et al. Negative association of the chemokine receptor ccr5 d32 polymorphism with systemic inflammatory response, extra-articular symptoms and joint erosion in rheumatoid arthritis, Arthritis Research & Therapy, vol. 11, no. 3, 2009. https://doi.org/10.1186/ar2733
[9] X. Jiao, M. Velasco-Velázquez, M. Wang, Z. Li, H. Rui, A. Peck, et al. Ccr5 governs dna damage repair and breast cancer stem cell expansion, Cancer Research, vol. 78, no. 7, p. 1657-1671, 2018. https://doi.org/10.1158/0008-5472.can-17-0915
[10] M. Velasco-Velázquez, X. Jiao, M. Fuente, T. Pestell, A. Ertel, M. Lisanti, et al. Ccr5 antagonist blocks metastasis of basal breast cancer cells, Cancer Research, vol. 72, no. 15, p. 3839-3850, 2012. https://doi.org/10.1158/0008-5472.can-11-3917
[11] T. Baltus, A. Kallaur, M. Lozovoy, H. Morimoto, F. Delongui, D. Alfieri, et al. Ccr5δ32 (rs333) polymorphism is associated with the susceptibility to systemic lupus erythematosus in female brazilian patients, Rheumatology International, vol. 36, no. 1, p. 7-15, 2015. https://doi.org/10.1007/s00296-015-3308-z
[12] E. Rzeszotarska, A. Sowińska, B. Stypińska, E. Walczuk, A. Wajda, A. Lutkowska, et al. The role of mecp2 and ccr5 polymorphisms on the development and course of systemic lupus erythematosus, Biomolecules, vol. 10, no. 3, p. 494, 2020. https://doi.org/10.3390/biom10030494
There are currently no reviews for this product.

