Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
On January 25, 2020, Prof Bin Cao's team published a research paper titled "Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China.". The paper revealed that the immune system of critical patients infected with SARS-CoV-2 (formerly known as: 2019-nCoV) exists a lethal cytokine storm. So what is cytokine storm? Why does the virus cause cytokine storm and its mechanism? Is there any treatments of cykine storm? In this article, we focus on the cytokine storm caused by virus infection. We will give you explaination from the following aspects:
Cytokine storm, also known as high cytokine disease, is the systemic expression of a healthy and vigorous immune system resulting in the release of more than 150 inflammatory mediators such as TNF-α, IL-1, IL-6, IL-12, IFN-α, IFN-β, IFN-γ, MCP-1, and IL-8. Both pro-inflammatory cytokines and anti-inflammatory cytokines are elevated in the serum, and the fierce and often lethal interplay of these cytokines is referred to as a "Cytokine Storm".
It is a severe excessive immune response caused by a positive feedback cycle between cytokines and immune cells. The symptoms are high fever, redness, swelling, extreme fatigue and nausea, which can be fatal in some cases. Cytokine storm is an important cause of acute respiratory distress syndrome and multiple organ failure (Figure 1).
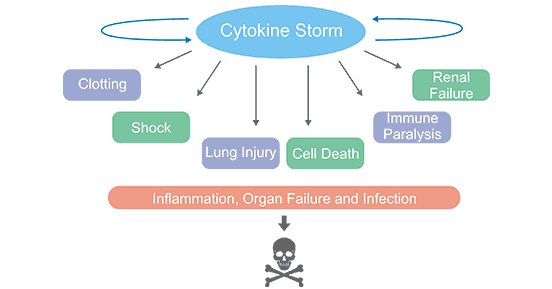
Figure 1. Cytokine Storm Causes Direct Organ Injury
After the virus enters the host target cells through the receptor-mediated endocytosis to proliferate in large numbers, it uses budding or induces programmed cell death to release more virus. These released virus are recognized by the pattern recognition receptors on the body's immune cells. Then the immune cells release a large number of cytokines through a series of signal transduction to activate more immune cells, which participate in the elimination of the virus.
However, as you know, immunity is a double-edged sword. When the body's immune activation attempts to remove exotic pathogenic microorganisms, it also leads to the body's own damage. If the amount of virus is large and the immunity is strong, a more severe local struggle will occur, causing local inflammation and cell damage, that is, a cytokine storm. At this time, the condition may worsen.
Taking Ebola virus as an example, it escapes the recognition of the immune system by lurking in host immature dendritic cells, macrophages, etc. After a large number of replications and rapid spread, it causes necrosis and decomposition of multiple organ cells. When the Ebola virus is released with the decomposed cells, the immune system will quickly recognize it. Due to the large amount of virus, the immune system is fully fired, releasing a large number of pro-inflammatory cytokines, tissue factors and vasoactive peptides. These released factors lead to penetrate the blood vessel wall and release a large amount of nitric oxide, causing secondary damage to the blood vessel wall and damaging the coagulation system. These reaction will cause the body to fever, internal bleeding, and eventually lead to multiple organ failure (Figure 2).
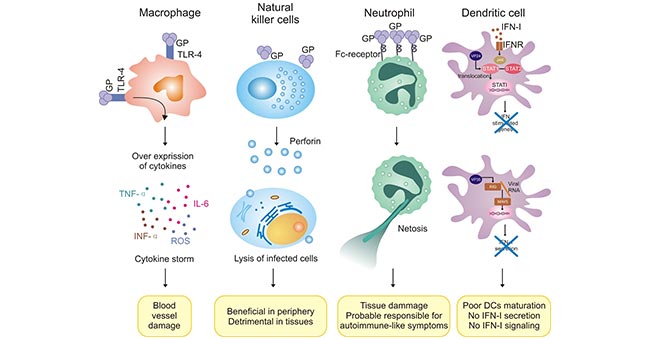
Figure 2. Abnormal Regulation of Innate Immune Cells in Ebola Virus Infection
Cytokine storm is common in viral infections, certain medications, and hematopoietic diseases. Cytokine storm is an important cause of acute respiratory distress syndrome (ARDS) and multiple organ failure. It is one of the important causes of death in many diseases, and it recently attractes more and more attention. In this article, we primarily focus on cytokine storm caused by virus infection. In addition to Ebola virus, dengue virus, highly pathogenic avian influenza virus (H5N1, H1H1, etc.), megavirus, smallpox virus, SARS virus, and MERS virus can cause cytokine storms.
SARS, also known as severe acute respiratory syndromes, is a major symptom of fever, dry cough, and chest tightness caused by SARS coronavirus infection. It began in December 2002. In terms of SARS-induced cytokine storm, Dr. Peiris of the University of Hong Kong found in autopsy that patients with severe SARS had significant damage to lung tissue, multinucleated giant cells in the alveoli, and alveolar macrophages that increased nuclear amphoteric staining cytoplasm.. These cells can secrete TNF, IL-1, TGF and other cytokines, and then induce fibroblast activation, extracellular matrix deposition and alveolar epithelial damage repair. Phagocytosis of red blood cells in the lung tissue suggests that cytokine regulation is out of control. It is speculated that SARS infection caused the release of many inflammatory mediators.
Zhiying Liu detected the presence of high concentrations of inflammatory and anti-inflammatory factors in cured and dead SARS patients. The high of IL-6, IL-8, and IL-10 suggest that the three cytokines play an important role in the progression of patients' disease. In the treatment of SARS patients, steroid hormones are commonly used to inhibit the release of cytokines, reduce the response and reduce mortality.
As mentioned on the article entilted 2019 Novel Coronavirus, the alignment between SARS-CoV-2 and 2002 SARS CoV has about 70% sequence similarity and 40% sequence similarity with MERS CoV. SARS-CoV-2 is a new strain of coronavirus that has never been found in humans before. Common signs of a person infected with a coronavirus include respiratory symptoms, fever, cough, shortness of breath, and dyspnea. In more severe cases, infection can cause pneumonia, severe acute respiratory syndrome, kidney failure, and even death. 2019-nCoV infection leads to a severe pneumonia epidemic. Most of the infected people are healthy people and young adults. The symptoms are similar to SARS. Some patients will suddenly change from mild to severe. It cannot be ignored because of the "cytokine storm".
Influenza virus induce mouse glial cell cytokine storm. Zhou Jianxiang et al. isolate and culture glial cells from the cerebral cortex of newborn mice and infect astrocytes with influenza viruses H1N1 and H3N2 in vitro at 6h and 24h respectively. The supernatant was harvested and the influenza virus were removed by ultrafiltration molecular retention. Conditional supernatants at different cultural time were used to stimulate astrocytes and microglia, respectively. RNA was extracted and reverse transcribed after 24 hours. Real-Time PCR was used to detect the pro-inflammatory factors (TNF-α, IL-1β, and IL- 6) and chemokines (IP-10, MCP-1, and MIP-1) .
This study indicated that the condition supernatant at different cultural time upregulates the proinflammatory factors TNF-α, IL-1β, IL-6 and chemokines IP-10, MCP-1, MIP-1 in normal glial cells. Up-regulation to varying degrees produces a cytokine cascade effect. The cytokine cascade effect caused by influenza viruses H1N1 and H3N2 infected astrocytes may be related to immunopathological damage.
EBV-associated lymphocytic proliferative diseases are associated with cytokine storms. CAEBV was nominated as EBV+LPD on a EBV-LPD seminar held at the National Institutes of Health on September 8-9, 2008. EBV+LPD is divided into B cell type (EBV+B-LPD) and T / NK cell type (EBV+T / NK-LPD). It is also called hemophilic syndrome (HPS). Kimura et al. Analyzed the virological differences and cytokine secretion in 39 patients with T-CAEBV and NK-CAEBV. And they found that IL-1β, IL-10 and IFN-γ are highly expressed in both serum, but the levels of IL-13 in patients with NK cell-type infection were higher than that of T-cells, and the serum of some patients who progressed to HPS expressed IL-1β and IFN-γ. In addition, the transcription of cytokines such as IL-1α, IL-1β, IL-10, IL-12p35, IL-13, IL-15, TNF-α, and IFN-γ in peripheral blood mononuclear cells of 19 CAEBV patients were increased.
Moreover, Ishii et al. found that monocytes can promote EBV-related NK / T cell proliferation and secrete LMP1 through IL-15 on the membrane, demonstrating the important role of IL-15 in the progression of EBV-LPD disease. SNK6 cell line highly expresses IFN-γ, IL-9 and IL-10. IL-10 indirectly promotes cell proliferation by promoting the secretion of LMP1 and CD25. Different types of EBV-LPD express different cytokines.
Accroding to the mechanism of the cytokine storm, the thinkings of drug development derive from the following principles:
Researchers have done a lot of work from the above three ideas, and studied various corticosteroids, PPAR agonists, S1P1 receptor agonists, COX inhibitors, anti-TNF antibodies, ACEI / ARB inhibitors, and OX40 inhibitors against cytokine storms. Of the above therapies, the most effective pneumonia-related cytokine storm therapy in animal experiments is the 1-phosphate sphingosine receptor 1 agonist (S1PR1).
Sphingosine-1-phosphate (S1p), a signaling sphingolipid with five subtypes of its receptors, are mainly expressed in vascular endothelial cells and lymphocytes in lung tissue. S1P1 agonists (CYM-5442 and RP-002) have been reported to protect mice from death caused by severe influenza infection through attenuating cytokines and inhibiting infiltration of innate immune cells.
In a mouse model infected with the 2009 H1N1 pandemic influenza, the S1P1 receptor agonist alone reduced deaths from lethal infections by more than 80%. In addition, the combination of oseltamivir can reduce mouse mortality by 96%. This is by far the best effect of using immune regulation strategies in the treatment of virus-induced cytokine storm.
At present, Novona's Siponimod, one of Spingosine-1-receptor modulator drugs, has been approved for the treatment of multiple sclerosis. So, can Siponimmod be used in severe pneumonia caused by SARS-CoV-2 virus infection? Compared to remdesivir, the approved cibonimod has better safety, and compared with the use of a large number of hormones in critically ill patients, the targeted cibonimod has smaller side effects, will it work better with antivirals like lopinavir / ritonavir? Let's wait and see for the next scientific research.
References
[1] Huang C, Wang Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [J]. Lancet, 2020 Jan 24.
[2] Parsi M, Dargan K. Hemophagocytic Lymphohistiocytosis Induced Cytokine Storm Secondary to Human Immunodeficiency Virus Associated Miliary Tuberculosis[J]. Cureus 2020 Jan 07;12(1).
[3] Benjamin G. Chousterman, et al. Cytokine storm and sepsis disease pathogenesis[J]. Seminars in Immunopathology. July 2017, Volume 39, Issue 5, pp 517–528.
[4] Huang KJ, Su IJ, et al. An interferon-gamma-related cytokine storm in SARS patients [J]. J. Med. Virol. 2005 Feb;75(2).
[5] Sun Y, Jin C, et al. Host cytokine storm is associated with disease severity of severe fever withthrombocytopenia syndrome[J]. INFECT DIS. 2012, 7 (206).
[6] IshiiH, Takahara M, et al. Monocytes enhance cell pro-liferation and LMP1 expression of nasalnatural killer/T-cell lympho-ma cells by cell contact-dependent interactionthrough membrane-bound IL-15 [J]. Int J Cancer. 2011, 130 (1): 48-58.


Comments
Leave a Comment