Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
At the AACR 2023 Annual Meeting, AbCellera, a Canadian biotech company, shows their latest research , focusing on MAGE-A4. They introduced the T cell inducer (TCE) platform, featuring a bispecific antibody that binds to both tumor-killing T cells and tumor targets, directing the immune system towards recognizing and eradicating cancer cells. By using TCE against pMHC with tumor-specific antigens, immune responses can be activated against the challenging MAGE-A4 tumor target.
MAGE-A4, part of the MAGE-As subfamily, is widely expressed in various malignant tumors and holds significant potential for immunotherapy. While MAGE-A1 and MAGE-A3 are extensively studied in the MAGE-A subfamily, other members receive less attention due to the challenge of obtaining specific antibodies. Researchers are now focused on developing monoclonal antibodies with enhanced specificity to reveal the potential of the MAGE family in tumor-specific immune studies.
1. What is Melanoma Antigen (MAGE)?
3. How's the Regulatory Mechanisms of MAGE-A4 in Tumors?
5. The Prospects for MAGE-A4 Clinical Research
6. CUSABIO MAGEA4 Recombinant Proteins & Antibodies for Research Use
The Melanoma antigen (MAGE) family is a large and complex group, categorized into two subclasses, MAGE-I and MAGE-II (Figure 1) [1]. MAGE-I antigens, also known as Tumor-Specific Antigens (TSAs), belong to a extensive family of cancer testis antigens, primarily found in germ cells and trophoblast cells. This group encompasses three subfamilies: MAGE-A, B, and C. On the other hand, MAGE-II antigens, present in normal human cells, consist of subfamilies MAGE-D, E, F, G, H, and L, and are distinct from cancerous testicular antigens. Among these, the MAGE-A subfamily comprises 15 members from MAGE-A1 to MAGE-A15, with many human tumors expressing at least one MAGE-A gene. Consequently, MAGE-A has garnered considerable attention as a tumor-specific antigen, proving to be a vital focus for the research of various tumors [1-5].
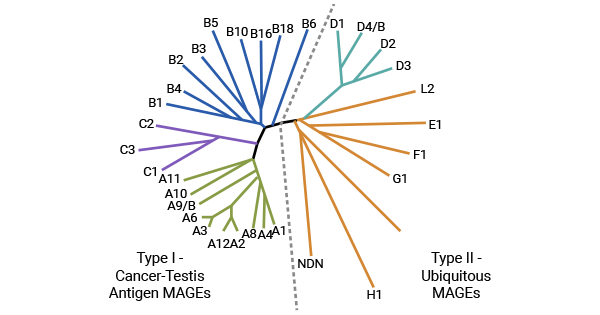
Figure 1. The MAGE family [1]
Melanoma-associated antigen 4 (MAGEA4 or MAGE-A, MAGE4) is a tumor/testis tissue antigen belonging to the MAGE-As family of protein isoforms. The MAGE-As subfamily is predominantly located in the region of the X chromosome, q28, spanning about 45 kb, with three exons (Figure. 2) [1]. MAGE-A encodes a protein of 309-319 amino acids. Intracellular processing of MAGE-A generates antigenic peptides that bind to HLA class I molecules, presenting complexes through MHC class I molecules to CD8+ T cells, thus eliciting a tumor-specific immune response in patients [6-8].
MAGE-A4 is exclusively expressed in normal tissues in the testis and placenta but is widely present in various cancer cells. As the first discovered carcinoembryonic antigen, the MAGE family has spurred research into specific immunotherapy against tumor cells, with a focus on the MAGE-A subfamily. Research has demonstrated that the MAGE-A gene activates specific T lymphocytes, instigating their attack on tumor cells. Given that over half of all tumors express MAGE genes, studying the MAGE-A family remains crucial for immune studies of tumors [9-11].
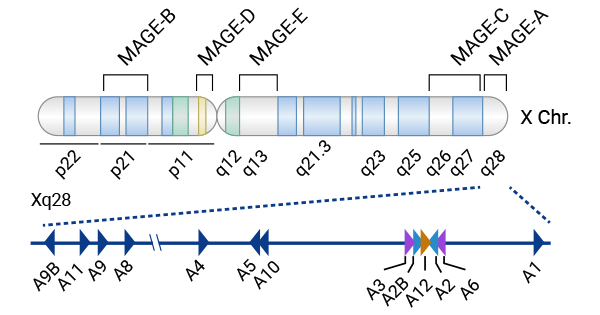
Figure 2. The MAGE-As subfamily mainly resides on the X chromosome's q28 region [1]
MAGE-A4 is distinctive within its family and is a favored target for tumor vaccines due to its ability to bind to specific MHC molecules. This binding activates T-cells, prompting them to eliminate tumor cells. Despite its significance, the precise regulatory mechanisms of MAGE-A4 in tumors remain largely unexplored. However, emerging evidence suggests its involvement in apoptosis and cell cycle processes [11-19].
Studies have revealed the association of MAGE-A4 with the oncogene P53, wherein its C-terminal fragment (MAGE-A4DeltaN1) triggers P53-dependent and P53-independent mechanisms by partially binding to Miz-1. This interaction boosts P53's transcriptional activity while reducing the levels of p21 (Cip1) transcript and protein. As an important oncogene regulating apoptosis and the cell cycle, MAGE-A4's biological function in inhibiting tumor progression underscores its role in protecting the organism from tumor assaults (Figure 3) [13]. Additionally, the Twist1 enhancer's non-directive binding to the promoter of MAGE-A4 leads to its amplification. However, other studies suggest that MAGE-A4 can activate the trans-lesion synthesis (TLS) pathway, hindering normal cell damage repair while selectively promoting DNA damage repair in chemotherapy cells, which ultimately helps tumor cells resist chemotherapy [11].
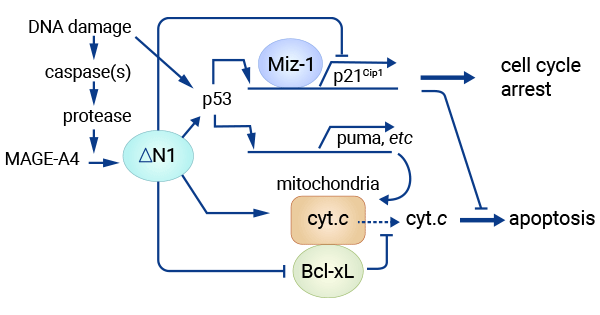
Figure 3. MAGE-A4 partially binds with Miz-1, activating P53-dependent and independent mechanisms. [13]
The MAGE-A family members are expressed in numerous tumor types, including hepatocellular carcinoma, non-small cell lung cancer, bladder cancer, vulvar cancer, colorectal tumors, salivary gland tumors, and cervical cancer [4-5, 20-21]. Recent research has identified the expression of MAGE-A4 in various malignant tumors such as breast cancer, glioma, esophageal squamous carcinoma, prostate cancer, thyroid cancer, and oral squamous cell carcinoma [10-11, 22-23]. This wide distribution suggests that MAGE-A4 may have important biological functions and clinical significance in a variety of tumor types.
It was found that in triple-negative breast cancer (TNBC), the positivity rate of MAGE-A4 was 35.21%, which was higher than that of non-triple-negative breast cancer. In addition, it was noted that MAGE-A4 expression was correlated with tumor clinical stage, and its positive expression rate decreased with higher clinical stage, which may play an inhibitory role in tumor progression. MAGE-A family members and NY-ESO-1 have been identified as tumor-associated antigens in breast cancer, which are associated with estrogen receptor (ER) expression was positively correlated.
Meanwhile, the expression of MAGE-As is associated with the poor prognostic indicator of HER-2, a poor prognostic indicator for breast cancer. In addition, MAGE-A4 can activate CD4+T cells in vivo and promote the body's immune response, which has the potential to kill tumor cells at the early stage of the tumor through immune response. These findings suggest that MAGE-A4 is expected to be a potential target for the treatment of TNBC [22].
MAGE-A4 expression in gliomas was found to be statistically significant compared with that in normal brain tissue. MAGE-A4 is not expressed in normal somatic cells outside of testicular tissue, which provides a theoretical basis for the use of MAGE-A4 as a specific target antigen in glioma immunotherapy. MAGE-A4 mRNA expression was significantly higher in high-grade gliomas (grades Ⅲ to Ⅳ) than in low-grade gliomas (grades I-II). This suggests a possible link between MAGE-A4 and glioma malignancy, making it a valuable indicator for assessing tumor severity and patient condition. MAGE-A4 was specifically expressed in glioma tissues and was significantly correlated with pathological grades, whereas it was not expressed in normal brain tissues. Therefore, MAGE-A4 could be an ideal target for immunotherapy of glioma [23, 25].
Using qPCR and immunohistochemistry for separate assays, the researchers found that in esophageal squamous carcinoma, the expression rate of MAGE-A4 was as high as 50%, while the expression level was lower in atypical tissues and normal esophageal mucosa. This finding highlights the strict tumor expression specificity of the MAGE-A4 in esophageal squamous carcinoma. Therefore, MAGE-A4 might be used as a specific diagnostic biomarker for esophageal squamous carcinoma, providing a strong basis for accurate clinical research. With the use of tumor-specific markers in clinical research, it is anticipated to positively impact the management of various cancer types, contributing to advanced research [27-28].
Research has highlighted the significant role of MAGE-A4 in various tumor types. For instance, in lung squamous carcinoma cell line H1703, silencing the MAGE-A4 gene using small RNA led to a 58% decrease in caspase-3 activity [28]. Similarly, therapeutic interventions involving MAGE-A4 antigenic peptides in rectal cancer patients led to a notable reduction in tumor growth rate and carcinoembryonic antigen levels [29].
Furthermore, an analysis of 187 non-small cell lung cancer patients revealed that MAGE-A4 expression in tissues was linked to a reduced human leukocyte antigen HLA and significantly lowered 5-year survival rates [30]. Differential expression of MAGE-4, MAGE-12, and NY-ESO-1 was observed in esophageal cancer tissues compared to adjacent normal tissues [31]. Notably, MAGE-A was found to be associated with prostate cancer, acting as a molecular bridge to enhance the transcriptional activity of AR and consequently promoting the growth of AR-dependent prostate cancer.
Presently, there are 19 drugs in clinical studies targeting MAGEA4. Among them, the most advanced is Afamitresgene Autoleucel (Ekiorunsay), a TCR cell therapy currently undergoing Phase III clinical trials for the treatment of synovial sarcoma, esophageal cancer, and mucinous liposarcoma, among others. Other drug types include bispecific antibodies, recombinant proteins, cellular therapies, fusion proteins, and T-cell therapies. Although the primary target of these drugs is MAGE-A4, some also target additional markers such as CD3, MAGEA8, NY-ESO-1, PRAME, SSX2, survivin, WT1, HLA-A24, CCL19, and IL-7.
The mechanism of action of drugs based on MAGEA4 targets is mainly to induce tumor cell apoptosis or inhibiting tumor growth and metastasis. Some also enhance immune responses or facilitate cell replacement. These drugs are investigated for various tumors, including melanoma, bladder cancer, and lung cancer, with potential indications in other diseases. Their development highlights the significance of MAGEA4 in tumor immunology research.
MAGEA4, a tumor/testis-specific antigen, shows significant involvement in various cancers, such as glioma, lung, esophageal, and prostate cancers. Studies indicate its role in tumor progression, cell apoptosis, and chemoresistance. Targeted therapies including T cell-based treatments and bispecific antibodies demonstrate promise in inducing apoptosis and inhibiting metastasis. Ongoing clinical trials highlight MAGEA4 as a valuable target in tumor immunology research, presenting potential for effective anti-cancer treatments.
To fully support researchers and pharmaceutical companies in their research on MAGEA4 in tumors and other diseases, CUSABIO presents MAGEA4 active proteins & antibodies to support your research on the mechanism of MAGEA4 or its potential clinical value.
CUSABIO MAGEA4 Protein
Recombinant Human Melanoma Antigen 4 (MAGEA4) (Active) Code: CSB-MP013330HU
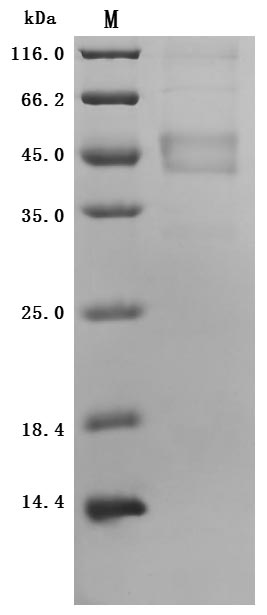
The high purity is greater than 90% as determined by SDS-PAGE.
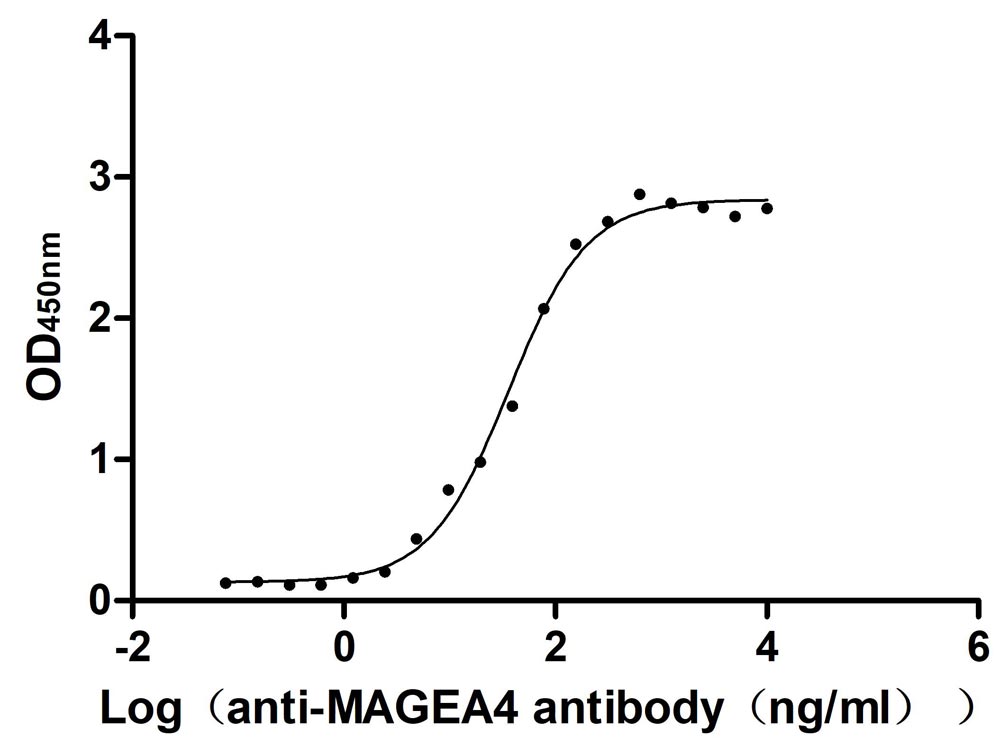
Immobilized Human MAGEA4 at 2 μg/ml can bind anti-MAGEA4 recombinant antibody. The EC50 is 30.33-43.10 ng/mL.
CUSABIO MAGEA4 antibody
MAGEA4 Monoclonal Antibody (Code: CSB-MA013330A0m)
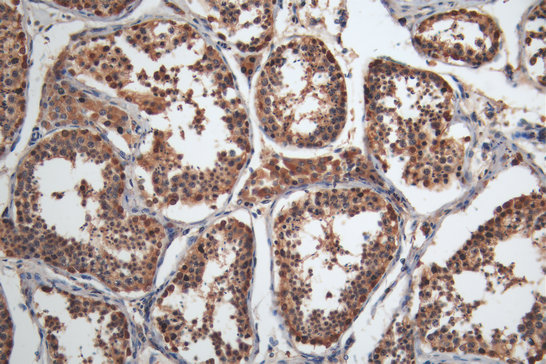
IHC image of CSB-MA013330A0m diluted at 1:200 and staining in paraffin-embedded human testis tissue performed on a Leica BondTM system.
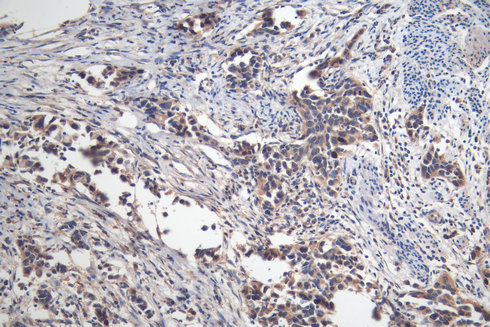
IHC image of CSB-MA013330A0m diluted at 1:200 and staining in paraffin-embedded human bladder cancer performed on a Leica BondTM system.
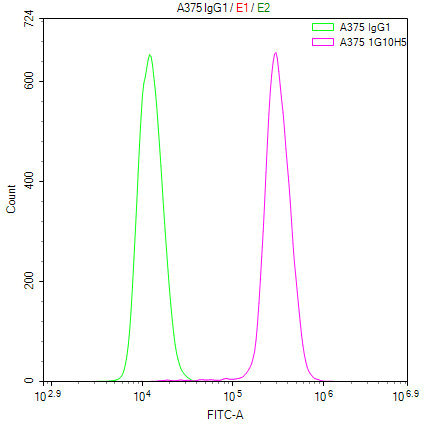
Overlay Peak curve showing A375 cells stained with CSB-MA013331A0m (red line) at 1:100.
References
[1] Lee, Anna K., and Patrick Ryan Potts. "A comprehensive guide to the MAGE family of ubiquitin ligases." Journal of molecular biology 429.8 (2017): 1114-1142.
[2] Chomez, Patrick, et al. "An overview of the MAGE gene family with the identification of all human members of the family." Cancer research 61.14 (2001): 5544-5551.
[3] Weon, Jenny L., and Patrick Ryan Potts. "The MAGE protein family and cancer." Current opinion in cell biology 37 (2015): 1-8.
[4] Meek, David W., and Lynnette Marcar. "MAGE-A antigens as targets in tumour therapy." Cancer letters 324.2 (2012): 126-132.
[5] Sang, Meixiang, et al. "MAGE-A family: attractive targets for cancer immunotherapy." Vaccine 29.47 (2011): 8496-8500.
[6] Aubry, Florence, et al. "MAGE‐A4, a germ cell specific marker, is expressed differentially in testicular tumors." Cancer: Interdisciplinary International Journal of the American Cancer Society 92.11 (2001): 2778-2785.
[7] Hagiwara, Yoshio, et al. "Consequences of point mutations in melanoma-associated antigen 4 (MAGE-A4) protein: Insights from structural and biophysical studies." Scientific reports 6.1 (2016): 25182.
[8] Sun, Qian, et al. "T-cell receptor gene therapy targeting melanoma-associated antigen-A4 by silencing of endogenous TCR inhibits tumor growth in mice and human." Cell death & disease 10.7 (2019): 475.
[9] Chambost, Hervé, et al. "Expression of gene MAGE-A4 in Reed-Sternberg cells." Blood, The Journal of the American Society of Hematology 95.11 (2000): 3530-3533.
[10] Kocher, Thomas, et al. "Prognostic relevance of MAGE‐A4 tumor antigen expression in transitional cell carcinoma of the urinary bladder: a tissue microarray study." International journal of cancer 100.6 (2002): 702-705.
[11] Gao, Yanzhe, et al. "A neomorphic cancer cell-specific role of MAGE-A4 in trans-lesion synthesis." Nature communications 7.1 (2016): 12105.
[12] Saito, Takuro, et al. "High expression of MAGE-A4 and MHC class I antigens in tumor cells and induction of MAGE-A4 immune responses are prognostic markers of CHP-MAGE-A4 cancer vaccine." Vaccine 32.45 (2014): 5901-5907.
[13] Sakurai, Toshiharu, et al. "A cleaved form of MAGE-A4 binds to Miz-1 and induces apoptosis in human cells." Journal of Biological Chemistry 279.15 (2004): 15505-15514.
[14] Cruz, Conrad R., et al. "Improving T-cell therapy for relapsed EBV-negative Hodgkin lymphoma by targeting upregulated MAGE-A4." Clinical Cancer Research 17.22 (2011): 7058-7066.
[15] Sanderson, Joseph P., et al. "Preclinical evaluation of an affinity-enhanced MAGE-A4-specific T-cell receptor for adoptive T-cell therapy." Oncoimmunology 9.1 (2020): 1682381.
[16] Takahashi, Norihiko, et al. "First clinical trial of cancer vaccine therapy with artificially synthesized helper/killer‐hybrid epitope long peptide of MAGE‐A4 cancer antigen." Cancer science 103.1 (2012): 150-153.
[17] Kageyama, Shinichi, et al. "Adoptive transfer of MAGE-A4 T-cell receptor gene-transduced lymphocytes in patients with recurrent esophageal cancer." Clinical Cancer Research 21.10 (2015): 2268-2277.
[18] Okumura, Satoshi, et al. "Chimeric antigen receptor T-cell therapy targeting a MAGE A4 peptide and HLA-A* 02: 01 complex for unresectable advanced or recurrent solid cancer: protocol for a multi-institutional phase 1 clinical trial." BMJ open 12.11 (2022): e065109.
[19] Kobayashi, Hiroshi, et al. "The biology of uterine sarcomas: a review and update." Molecular and clinical oncology 1.4 (2013): 599-609.
[20] Tsai, Jong-Rung, et al. "Differential expression profile of MAGE family in non-small-cell lung cancer." Lung cancer 56.2 (2007): 185-192.
[21] Dhodapkar, Madhav V., et al. "Expression of cancer/testis (CT) antigens MAGE-A1, MAGE-A3, MAGE-A4, CT-7, and NY-ESO-1 in malignant gammopathies is heterogeneous and correlates with site, stage and risk status of disease." Cancer Immunity 3.1 (2003).
[22] Cabezon, Teresa, et al. "Proteomic profiling of triple-negative breast carcinomas in combination with a three-tier orthogonal technology approach identifies Mage-A4 as potential therapeutic target in estrogen receptor negative breast cancer." Molecular & Cellular Proteomics 12.2 (2013): 381-394.
[23] Two-Pronged, A. "471. CMV-Specific HER2-Redirected T Cells for the Adoptive Immunotherapy of Glioblastoma." Molecular Therapy 18 (2010): 1.
[24] Guo, Liru, et al. "The expression and clinical significance of melanoma‑associated antigen‑A1,‑A3 and‑A11 in glioma." Oncology letters 6.1 (2013): 55-62.
[25] Ebrahimabadi, S., et al. "MAGE-A4-CAR-NK CELL THERAPY FOR THE TREATMENT OF SOLID TUMORS." Hematology, Transfusion and Cell Therapy 45 (2023): S534-S535.
[26] Chen, Xiaohua, et al. "Analysis of the function of MAGE-A in esophageal carcinoma by bioinformatics." Medicine 98.21 (2019).
[27] Ueda, Shugo, et al. "NY-ESO-1 antigen expression and immune response are associated with poor prognosis in MAGE-A4-vaccinated patients with esophageal or head/neck squamous cell carcinoma." Oncotarget 9.89 (2018): 35997.
[28] Peikert, Tobias, et al. "Melanoma antigen A4 is expressed in non–small cell lung cancers and promotes apoptosis." Cancer research 66.9 (2006): 4693-4700.
[29] Liu, Fangfang, et al. "A study of protein expression of MAGE-A3, MAGE-A4 and MAGE-A10 genes in colorectal carcinoma and its clinical significance." Chinese Journal of General Surgery (2012): 37-39.
[30] Baba, Tetsuro, et al. "Clinical significance of human leukocyte antigen loss and melanoma-associated antigen 4 expression in smokers of non-small cell lung cancer patients." International journal of clinical oncology 18 (2013): 997-1004.
[31] Zhang, Yujie, Yuxin Zhang, and Li Zhang. "Expression of cancer–testis antigens in esophageal cancer and their progress in immunotherapy." Journal of cancer research and clinical oncology 145 (2019): 281-291.
[32] Bergeron, Alain, et al. "High frequency of MAGE‐A4 and MAGE‐A9 expression in high‐risk bladder cancer." International Journal of Cancer 125.6 (2009): 1365-1371.


Comments
Leave a Comment