Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
C-C chemokine receptor 4 (CCR4) is an important member of the G protein-coupled receptor family, primarily involved in the recruitment, migration, and functional regulation of immune cells. As a key surface receptor on T helper 2 (Th2) cells and Regulatory T cells (Treg), CCR4 recognizes its ligands CCL17 (TARC) and CCL22 (MDC) to play critical roles in immune homeostasis maintenance, inflammatory responses, and immune tolerance formation. Recent studies have demonstrated that abnormal expression or functional imbalance of CCR4 is closely associated with multiple diseases, particularly hematological malignancies, solid tumors, autoimmune diseases, and chronic inflammatory disorders. CCR4 not only remodels the local immune microenvironment by recruiting immunosuppressive Treg cells but also directly participates in the regulation of tumor cell migration, invasion, and drug resistance. With the continuous advancement of CCR4-targeted antibodies, small molecule antagonists, and cell therapy strategies, this receptor has become an important research target in the fields of immunotherapy and inflammatory intervention.
CCR4 is a typical seven-transmembrane G protein-coupled receptor, mainly expressed on the surface of various immune cells including Th2 cells, Treg cells, dendritic cells, macrophages, and cytokine-induced killer cells [4–7]. In healthy individuals, CCR4 is often regarded as an important marker for Th2, Th17, and Treg cells [4], while its abnormal expression in various tumor cells is closely associated with poor prognosis [8–10]. The main ligands of CCR4 are CCL17 (TARC) and CCL22 (MDC), which are produced by multiple cell types including dendritic cells and macrophages. They play important regulatory roles in inflammatory and tumor microenvironments by recruiting CCR4-positive immune cells [6–8]. In the tumor microenvironment, M2-type macrophages can significantly enhance CCL17 secretion, thereby promoting tumor cell migration, invasion, and stemness maintenance [8]. Following ligand-receptor binding, CCR4 activates multiple signaling pathways and exhibits significant functional diversity across different cell types and disease contexts.
CCR4 primarily mediates downstream signal transduction through Gαi proteins. Upon ligand binding, Gβγ subunits activate Rho kinase and p38 MAPK pathways, regulating cytoskeletal rearrangement, chemotactic migration, and inflammatory responses [13]. Additionally, in different pathological environments, CCR4 can also influence cell survival, metabolism, and drug resistance through signaling pathways such as PI3K/AKT [11,12].
β-arrestin2 plays an important role in CCR4 signal transduction, participating in both receptor internalization and mediating independent signaling cascades. In allergic inflammation models, the CCL22-CCR4-β-arrestin2 axis has been demonstrated to play a critical role in Th2 cell chemotaxis and inflammation exacerbation [13]. Different ligands may exhibit biased signal activation patterns in specific cellular environments, providing new perspectives for targeted intervention [14].
CCR4 is an important regulator of chemotaxis for Th2 and Treg cells. In the tumor microenvironment, enrichment of CCR4⁺ Treg cells is closely associated with immunosuppression and poor prognosis [15]. Furthermore, CCR4 is involved in the functional regulation of CIK cells, dendritic cells, and macrophages, exhibiting dual roles in anti-tumor immunity, inflammatory responses, and immune tolerance formation.
CCR4 regulates tumor cell migration, invasion, epithelial-mesenchymal transition, and drug resistance through multiple pathways including ERK/AKT and EZH2-DNMT3A [3,8,16], further highlighting its central role in tumor progression.
During thymic development and central tolerance establishment, CCR4 and CCR7 play complementary roles at different stages and in distinct cell subpopulations, collectively ensuring effective clearance of self-reactive T cells [17].
CCR4 is highly expressed in various T cell-derived hematological malignancies, particularly with well-defined pathological significance in adult T cell leukemia/lymphoma (ATL) and cutaneous T cell lymphoma (CTCL). CCR4⁺ tumor cells can achieve directional migration and tissue infiltration through their ligands CCL17 and CCL22, while evading immune surveillance. Clinical studies have shown that high expression of CCR4 is usually closely associated with disease progression, increased invasiveness, and poor prognosis. The humanized anti-CCR4 monoclonal antibody Mogamulizumab, developed based on this characteristic, effectively eliminates CCR4⁺ tumor cells through antibody-dependent cell-mediated cytotoxicity (ADCC) and simultaneously depletes immunosuppressive Treg cells, thereby improving anti-tumor immune responses [2,18]. This drug has been approved for relapsed or refractory CTCL and peripheral T cell lymphoma, validating the clinical feasibility of CCR4 as a therapeutic target.
In addition to hematological malignancies, CCR4 also plays important roles in various solid tumors, including hepatocellular carcinoma, lung adenocarcinoma, breast cancer, and colorectal cancer. Studies have found that tumor-associated macrophages and dendritic cells can secrete large amounts of CCL17 and CCL22, selectively recruiting CCR4⁺ Treg cells to the tumor microenvironment, leading to local immunosuppression and weakened anti-tumor immune responses [8,15]. Furthermore, some solid tumor cells themselves express CCR4, and its activation can promote tumor cell proliferation, migration, and epithelial-mesenchymal transition through signaling pathways such as PI3K/AKT and ERK, thereby enhancing invasiveness and metastatic potential [3,8]. These findings provide a theoretical basis for the application of CCR4-targeted therapy in solid tumors and have promoted the exploration of combination strategies of CCR4 antagonists with immune checkpoint inhibitors [19,20].
The role of CCR4 in inflammatory and autoimmune diseases is mainly closely related to the migration of Th2 and Treg cells. In diseases such as rheumatoid arthritis, atopic dermatitis, and systemic lupus erythematosus, abnormal activation of the CCR4-CCL17/CCL22 axis can lead to excessive accumulation of immune cells in target tissues, thereby exacerbating inflammatory responses and tissue damage [1]. In some disease contexts, recruitment of CCR4⁺ Treg cells may have dual effects: on one hand, it helps inhibit excessive inflammation, while on the other hand, it may promote immune imbalance and delay tissue repair in chronic inflammatory states. This context-dependent functionality also suggests that CCR4-targeted interventions need to fully consider disease stage and immune status.
In recent years, the role of CCR4 in metabolic diseases has gradually attracted attention. In obesity and its related complications, CCR4 and its ligands are closely associated with chronic low-grade inflammation in adipose tissue and vascular endothelial dysfunction. CCR4-mediated immune cell recruitment may participate in the development of insulin resistance and metabolic disorders, providing a new research perspective for the cross-regulatory mechanisms between inflammation and metabolism.
In HTLV-1 and HIV-1 infections, CCR4⁺ CD4⁺ T cells are considered important viral reservoirs. High expression of CCR4 is not only associated with persistent viral presence but may also affect immune reconstitution and disease progression [4,21]. These findings suggest that CCR4 has potential intervention value in the immunopathological processes associated with viral infections.
Animal experimental studies have shown that CCR4 and its ligands play regulatory roles in the development and progression of neuropathic pain. CCR4 antagonists can significantly alleviate pain behaviors and enhance the analgesic efficacy of opioid analgesics [22], providing a new research direction for multi-target combination therapy of chronic pain.
In recent years, significant progress has been made in the research and development of CCR4-targeted drugs, covering multiple drug types from monoclonal antibodies, small molecule chemical drugs to CAR-T cell therapies. Among them, Mogamulizumab, as a representative CCR4 antagonist, has been approved for marketing for indications including mycosis fungoides, Sézary syndrome, and peripheral T cell lymphoma. Other investigational drugs such as Tivumecirnon Besylate and Autologous CCR4 CAR-T cells are in Phase 2 and Phase 1 clinical stages, mainly targeting malignant tumors such as metastatic gastric cancer, advanced cancer, and T cell lymphoma. In addition, multiple preclinical research projects are exploring the potential of CCR4 antagonists in various diseases including sepsis, liver cancer, asthma, rhinitis, anemia, and stroke. Overall, the R&D of CCR4-targeted drugs shows a diversified development trend, with oncology remaining the main research direction while expanding to other disease fields.
| Drug | Mechanism of Action | Drug Type | Indications in Development | Research Institutions | Highest R&D Phase |
|---|---|---|---|---|---|
| Mogamulizumab | CCR4 Antagonist | Monoclonal Antibody | Mycosis Fungoides | Sézary Syndrome | Peripheral T-cell Lymphoma, etc. | Kyowa Kirin Holdings BV | Kyowa Kirin, Inc | Approved for Marketing |
| Tivumecirnon Besylate | CCR4 Antagonist | Small Molecule Drug | Metastatic Gastric Cancer | Advanced Cancer | Rapt Therapeutics, Inc. | Hanmi Pharmaceutical Co., Ltd. | Phase 2 Clinical Trial |
| Autologous CCR4 CAR T cells (NCI) | CCR4 Modulators | Autologous CAR-T | - | National Cancer Institute | Phase 1 Clinical Trial |
| DB07845 | CCR4 Antagonist | Small Molecule Drug | Sepsis | Jiaxing Hospital of Traditional Chinese Medicine | Preclinical |
| CCR4-351 | CCR4 Antagonist | Small Molecule Drug | Adult T-cell Leukemia/Lymphoma | Tumor | Albert Einstein College of Medicine, Inc. | Rapt Therapeutics, Inc. | Preclinical |
| NTX-471 | CCR4 Modulators | CD47 Modulators | mRNA-encoded Bispecific Antibody | Anemia | Nutcracker Therapeutics, Inc. | Preclinical |
| CCR4 Inhibitor (ChemoCentryx) | CCR4 Antagonist | Small Molecule Drug | Asthma | Rhinitis | ChemoCentryx, Inc. | Preclinical |
| CCR4 Antagonist (Aurigene) | CCR4 Antagonist | Chemical Drug | Tumor | Aurigene Oncology Ltd. | Preclinical |
| BJY-809 | CCR4 Antagonist | Small Molecule Drug | Liver Cancer | Bajiayi Pharmaceutical Co., Ltd. | Preclinical |
| SSmall molecule therapeutic (Collaboration Pharmaceuticals) | CCR3 Antagonist | CCR4 Antagonist | Small Molecule Drug | Stroke | Collaborations Pharmaceuticals, Inc. | Preclinical |
| TQB-2619 | CCR4 Antagonist | Biological Drug | Chronic Lymphocytic Leukemia | T-cell Lymphoma | Zhengda Tianqing Pharmaceutical Group Co., Ltd. | Preclinical |
(Data as of March 11, 2026, sourced from Synapse)
CUSABIO provides CCR4 recombinant proteins and antibody products to support your mechanistic research and targeted drug development.
● CCR4 Recombinant Proteins
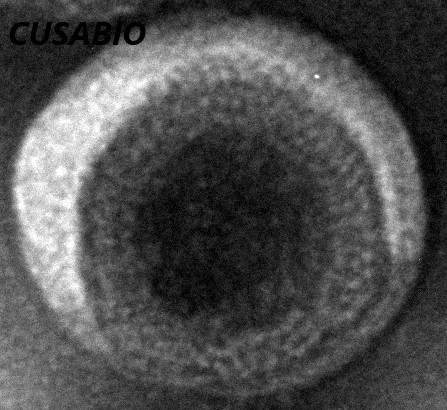
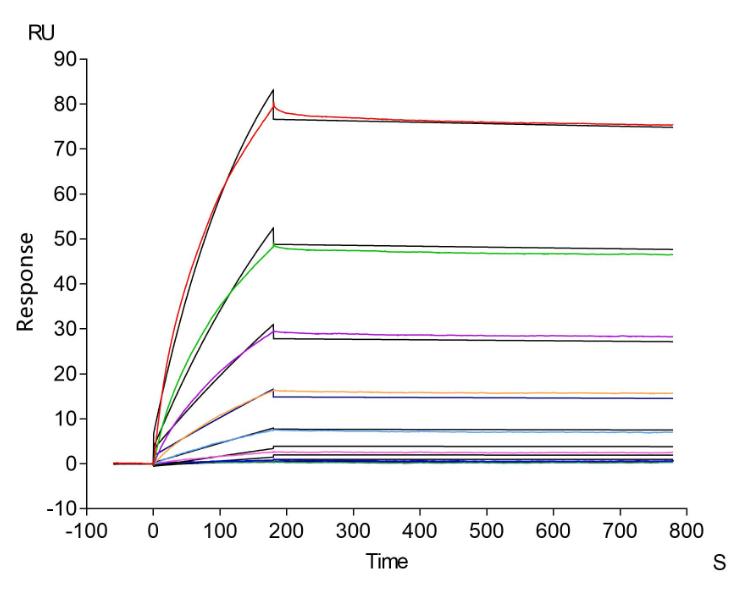
Recombinant Human C-C chemokine receptor type 4 (CCR4)-VLPs (Active); CSB-MP004843HU
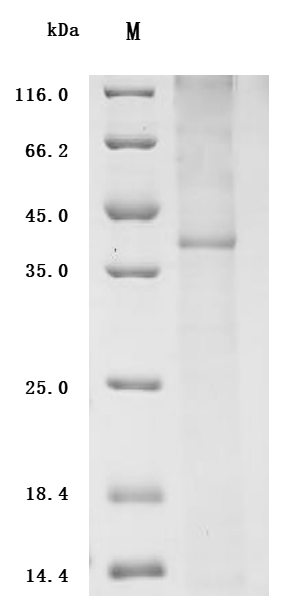
Recombinant Human C-C chemokine receptor type 4 (CCR4) (Active); CSB-CF004843HU
● CCR4 Antibodies
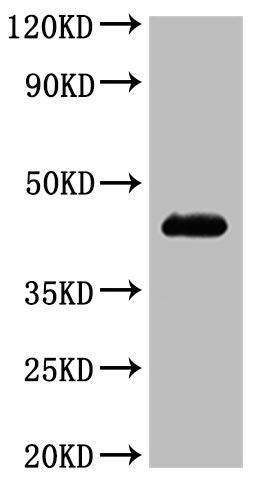
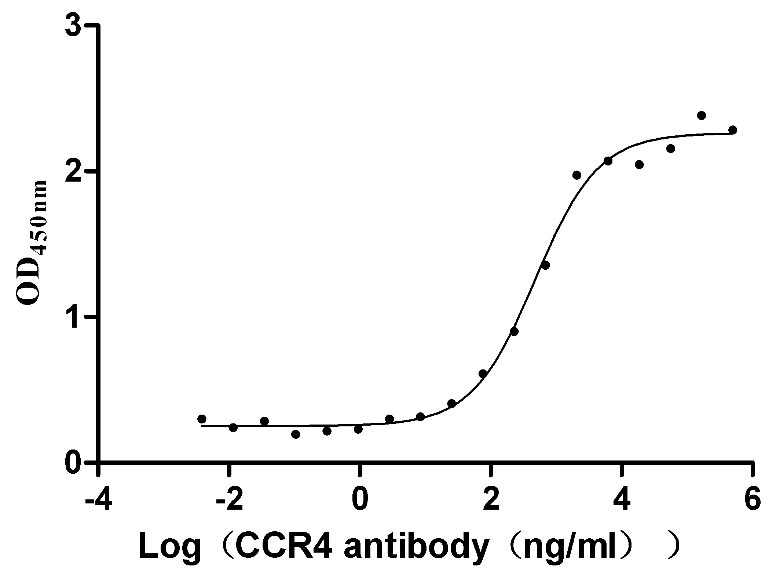
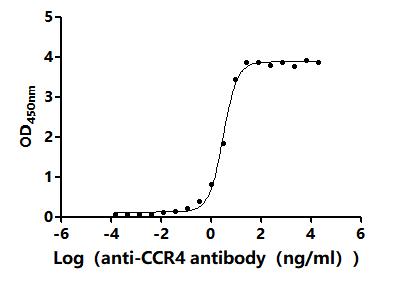
CCR4 Recombinant Monoclonal Antibody; CSB-RA004843MA01HU
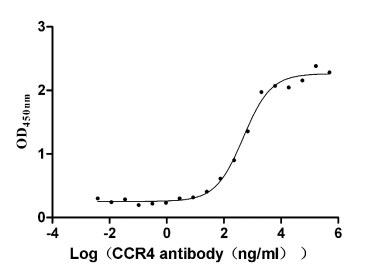
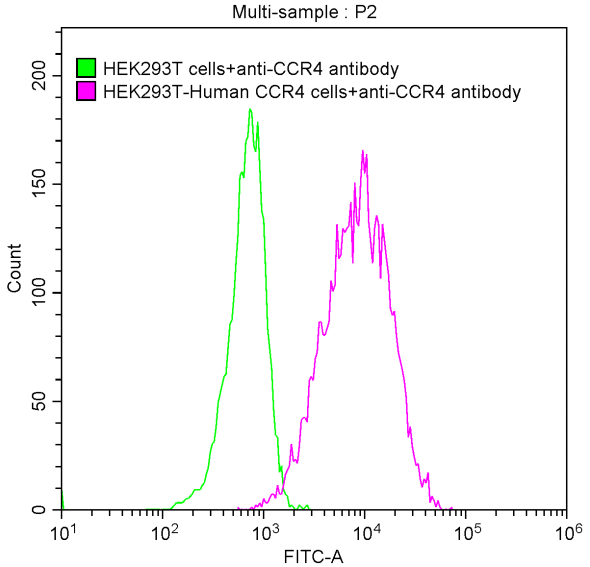
CCR4 Antibody; CSB-PA004843LA01HU
References
[1] Kayoko Hase, K. Tani, Teruki Shimizu, Y. Ohmoto, K. Matsushima, S. Sone.(2001). Increased CCR4 expression in active systemic lupus erythematosus.
[2] Kenji Ishitsuka, Tomoharu Yasukawa, Yukie Tsuji.(2024). Safety and effectiveness of mogamulizumab in relapsed or refractory CC chemokine receptor 4‐positive peripheral T‐cell lymphoma and relapsed or refractory cutaneous T‐cell lymphoma: A post‐marketing surveillance in Japan.
[3] Xi Cheng, Huo Wu, Zhi-Jian Jin, Ding Ma, Stanley Yuen, Xiaoqian Jing, Minmin Shi, B. Shen, C. Peng, R. Zhao, Wei-hua Qiu.(2017). Up-regulation of chemokine receptor CCR4 is associated with Human Hepatocellular Carcinoma malignant behavior.
[4] Y. Yamano, N. Araya, Tomoo Sato, A. Utsunomiya, Kazuko Azakami, D. Hasegawa, Toshihiko Izumi, Hidetoshi Fujita, S. Aratani, N. Yagishita, Ryoji Fujii, K. Nishioka, S. Jacobson, T. Nakajima.(2009). Abnormally High Levels of Virus-Infected IFN-γ+CCR4+CD4+CD25+ T Cells in a Retrovirus-Associated Neuroinflammatory Disorder.
[5] C. Carola, Andrew Salazar, C. Rakers, F. Himbert, Q. Do, P. Bernard, Joerg von Hagen.(2021). A Cornflower Extract Containing N-Feruloylserotonin Reduces Inflammation in Human Skin by Neutralizing CCL17 and CCL22 and Inhibiting COX-2 and 5-LOX.
[6] Yongjian Dong, Shuhui Gao, Xue-fang Zhang, Jing Kou, Jing Liu, Ting Ye, Han Shen.(2021). CCL17 and CCL22 induce CCR4 receptor expression and promote cytokine-induced killer cells migration.
[7] Inés Lecoq, K. Kopp, M. Chapellier, Panagiotis Mantas, E. Martinenaite, Maria Perez-Penco, Lars Rønn Olsen, M. Zocca, A. Wakatsuki Pedersen, M. Andersen.(2022). CCL22-based peptide vaccines induce anti-cancer immunity by modulating tumor microenvironment.
[8] Chun Jin, Liangliang Lu, Jian Gao, Ling Chen.(2024). M2-like Macrophages-derived CCL17 Promotes Esophageal Squamous Cell Carcinoma Metastasis and Stemness via Activating CCR4-mediated ERK/PD-L1 Pathway..
[9] A. Maolake, K. Izumi, K. Shigehara, Ariunbold Natsagdorj, H. Iwamoto, S. Kadomoto, Yuta Takezawa, Kazuaki Machioka, K. Narimoto, M. Namiki, Wen-Jye Lin, Guzailinuer Wufuer, A. Mizokami.(2016). Tumor-associated macrophages promote prostate cancer migration through activation of the CCL22–CCR4 axis.
[10] W. Gan, Baoye Sun, Zhangfu Yang, Cheng Ye, Zhutao Wang, Cheng Zhou, Guo-Qiang Sun, Yong Yi, Shuang-Jian Qiu.(2024). Enhancing hepatocellular carcinoma management: prognostic value of integrated CCL17, CCR4, CD73, and HHLA2 expression analysis.
[11] Lichao Zhang, Xiaoqing Lu, Yuanzhi Xu, Xiaoqin La, Jinmiao Tian, Aiping Li, Hanqing Li, Changxin Wu, Yanfeng Xi, Guisheng Song, Zhaocai Zhou, Wenqi Bai, Liwei An, Zhuoyu Li.(2023). Tumor-associated macrophages confer colorectal cancer 5-fluorouracil resistance by promoting MRP1 membrane translocation via an intercellular CXCL17/CXCL22–CCR4–ATF6–GRP78 axis.
[12] Shuixiang Deng, Peng Jin, P. Sherchan, Shengpeng Liu, Yuhui Cui, Lei Huang, John H. Zhang, Ye Gong, Jiping Tang.(2021). Recombinant CCL17-dependent CCR4 activation alleviates neuroinflammation and neuronal apoptosis through the PI3K/AKT/Foxo1 signaling pathway after ICH in mice.
[13] Rui Lin, Y. Choi, David A Zidar, Julia K. L. Walker.(2018). β‐Arrestin‐2‐Dependent Signaling Promotes CCR4‐mediated Chemotaxis of Murine T‐Helper Type 2 Cells.
[14] H. Lim, J. R. Lane, Meritxell Canals, M. Stone.(2021). Systematic Assessment of Chemokine Signaling at Chemokine Receptors CCR4, CCR7 and CCR10.
[15] Tania Sarkar, Subhanki Dhar, D. Chakraborty, Subhadip Pati, S. Bose, A. Panda, Udit Basak, S. Chakraborty, S. Mukherjee, A. Guin, Kuladip Jana, Diptendra K. Sarkar, Gaurisankar Sa.(2022). FOXP3/HAT1 Axis Controls Treg Infiltration in the Tumor Microenvironment by Inducing CCR4 Expression in Breast Cancer.
[16] Li Zhang, Sijuan Tian, Jie Chang, Shimin Quan, Ting Yang, Minyi Zhao, Li Wang, Xiaofeng Yang.(2024). Activation of the CCL22/CCR4 causing EMT process remodeling under EZH2-mediated epigenetic regulation in cervical carcinoma.
[17] Y. Li, J. Srinivasan, Hilary J. Selden, Lauren I. R. Ehrlich.(2023). CCR4 and CCR7 differentially regulate thymocyte localization with distinct outcomes for central tolerance.
[18] Z. Marušić, E. Calonje.(2021). Skin adnexal tumours in a tertiary dermatopathology service.
[19] Do-Youn Oh, Min-Hee Ryu, Jun-Eul Hwang, Jaeyong Cho, D. Y. Zang, Sang Cheul Oh, J. Lee, Keun-Wook Lee, S. Rha, B. Shim, William Ho, M. Chisamore, Paul Dong Rhee, Sooa Jung, Taewan Kim, Jiyeon Yoon, Hosung Jang, E. Baek, Young-Su Noh.(2025). A phase 2 study to assess the safety and efficacy of FLX475 (tivumecirnon) combined with pembrolizumab in patients with advanced or metastatic gastric cancer..
[20] Adam Grant, Juraj Adamik, Jingtao Qiu, Jacob Wert, Molly Grandcolas, S. Jacobson, R. Goyal, William Ho, Shoji Ikeda, Marvin Au, Damian L Trujillo, M. Chisamore, D. Nagata, M. S. Ghomi, D. Brockstedt, P. Kassner, George E. Katibah.(2024). Abstract 2485: A combined mregDC and Treg signature associates with antitumor efficacy of CCR4 antagonist tivumecirnon FLX475.
[21] Y. Mahnke, K. Fletez-Brant, I. Sereti, M. Roederer.(2016). Reconstitution of Peripheral T Cells by Tissue-Derived CCR4+ Central Memory Cells Following HIV-1 Antiretroviral Therapy.
[22] J. Bogacka, Katarzyna Ciapała, K. Pawlik, K. Kwiatkowski, J. Dobrogowski, A. Przeklasa-Muszyńska, J. Mika.(2020). CCR4 Antagonist (C021) Administration Diminishes Hypersensitivity and Enhances the Analgesic Potency of Morphine and Buprenorphine in a Mouse Model of Neuropathic Pain.


Comments
Leave a Comment