Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
Figure 1 AIDS Red Ribbon
Human Immunodeficiency Virus (HIV) is a lentivirus that belongs to the class of retroviruses. HIV is a virus that attacks the body's immune system. It takes CD4 T lymphocytes, the most important cells in the human immune system, as the main target of attack, and destroys the cells in large amounts, making the human body lose its immune function. Therefore, the human body is susceptible to various diseases and can develop malignant tumors.
In 1981, the human immunodeficiency virus was first discovered in the United States.
Since the discovery of HIV, the genome and protein of human immunodeficiency virus have been the subject of extensive research [1] [2]. As early as 1985, the sequence of the HIV genome has been reported [3] [4] [5].
The International Classification of Diseases-10 (ICD-10) of acquired immunodeficiency syndrome (AIDS) is B24.x01. Two types of HIV have been identified: HIV-1 and HIV-2. There are differences between HIV type 1 and HIV type 2, and their nucleic acid sequences are only 40% homologous.
HIV-1 originated from the chimpanzee common chimpanzee, and HIV-2 originated from the white-collared mangabey [6].
It is divided into four types: Group M, Group N, Group O, Group P.
"M" means "major", which is the most common type of HIV, with more than 90% of HIV/AIDS cases originating from the M group infected with HIV-1. The M group is further subdivided into branches, called subtypes. See Table 1 for details.
Table 1 Different subtypes of Group M and major distributions
| Subtypes | Main distribution |
|---|---|
| Subtype A | West Africa |
| Subtype B | Europe, the Americas, Japan, and Australia, Middle East and North Africa |
| Subtype C | Southern Africa, Eastern Africa, India, Nepal, and parts of China. |
| Subtype D | Only seen in Eastern and central Africa. |
| Subtype E | Southeast Asia (dominant form for heterosexuals) |
| Subtype F | Central Africa, South America and Eastern Europe. |
| Subtype G | Africa and central Europe. |
| Subtype H | Be limited to central Africa. |
| Subtype I | / |
| Subtype J | North, Central and West Africa, and the Caribbean |
| Subtype K | Be limited to the Democratic Republic of Congo and Cameroon. |
There is also a "cyclic recombination form", CRFs derived from recombination between different subtypes of viruses. For example, CRF12_BF is a recombination between subtypes B and F.
This is an HIV-1 variant that was identified and isolated from a Cameroonian woman who died of AIDS in 1998.
The O ("outsider") group is usually not common in areas outside the western part of Central Africa. According to reports, this is the most common in Cameroon.
In 2009, it was separated from a Cameroonian woman living in France. The scientists who reported the sequence placed it in a proposed group P, "waiting for further human case identification".
The vast majority of people living with HIV live in low - and middle-income countries. Africa has the world's largest number of people living with HIV/AIDS, and southern Africa is even worse. South and Southeast Asia are the second worst affected areas after Sub-Saharan Africa. The development of HIV risk environments [7] has been shaped by social-structural, economic and political factors specific to each context.
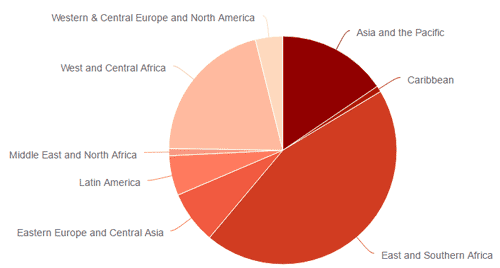
Figure 2 New HIV infections (all ages)-by region
HIV outbreak: By the end of 2016, about 36.7 million people worldwide were living with HIV. Of these, 2.1 million are children (under 15 years of age). In 2017, 19.6 million people were living with HIV in eastern and southern Africa, 6.1 million in western and central Africa, 5.2 million in Asia and the Pacific, and 2.2 million in western and central Europe and North America, 1.8 million people were living with HIV in Latin America, 1.4 million people were living with HIV in Eastern Europe and central Asia, 2.2 million people were living with HIV in Middle East and North Africa.
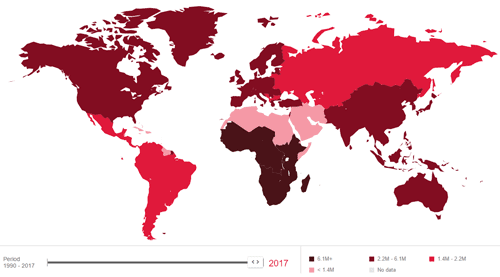
Figure 3 New trends in HIV infection in 2010-2017
AIDS breakthrough: Since 2010, the percentage change in AIDS-related deaths has fallen by 34%, the percentage change in the number of new HIV infections has fallen by 18%.
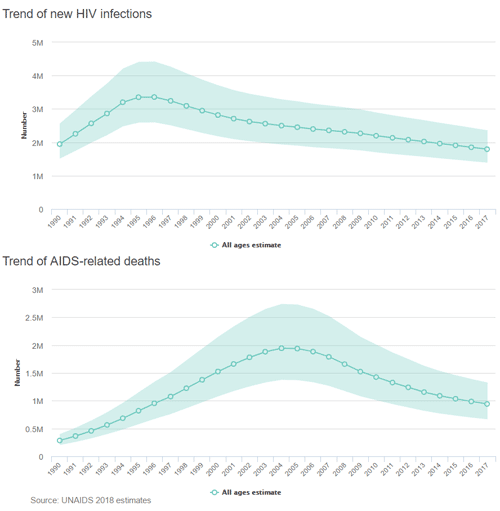
Figure 4 Trend of new HIV infections and AIDS-related deaths
More specific data can be found in the UNAIDS: http://aidsinfo.unaids.org./
At present, this international response to AIDS is unprecedented because resources are more committed than any other health cause [8]. This is called the AIDS exceptionalism.
The human immunodeficiency virus is approximately 120 nanometers in diameter and is generally spherical. It mainly includes the viral envelope, and the protein gp120 and gp41 (transmembrane protein). Inward is a spherical matrix formed of protein p17, and a semi-conical capsid formed by protein p24. The capsid contains viral RNA genomes, enzymes (reverse transcriptase, integrase, protease), and other components from host cells (such as tRNAlys3, which acts as a primer for reverse transcription).
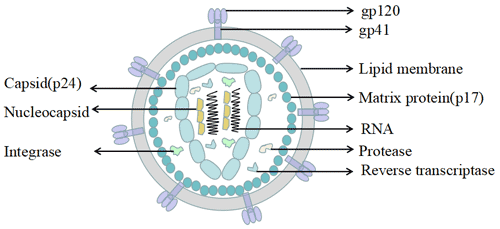
Figure 5 The structure of HIV
The viral genome is two identical positive strand RNAs, each of which is about 9.2 -9.8 kb. Both ends are long terminal repeats (LTR), containing cis-regulated sequences that control the expression of provirus. It has been demonstrated that LTR has promoters and enhancers and contains negative regulatory regions. The sequences between LTR encode at least nine proteins, which can be divided into three types: structural proteins, regulatory proteins and auxiliary proteins.
Compared with HIV-1, the HIV-2 gene does not contain the VPU gene, but has an unexplained VPX gene.
HIV-infected persons are the source of infection. HIV has been isolated from blood, semen, vaginal secretions, milk, etc.
The ability of HIV to survive in vitro is extremely poor, it is not resistant to high temperatures. So shaking hands, hugging, kissing, swimming, mosquito bites, sharing cutlery, coughing or sneezing, daily contact, etc. will not spread.
The following are the three main modes of communication [10]:
HIV is present in the semen and vaginal secretions of infected people. Sexual behavior can easily cause minor skin mucosa damage, and the virus can be infected through the damaged area into the blood.
The human body is exposed to blood or blood products containing HIV, intravenous drug use, and transplant tissues and organs of infected patients are at risk of contracting AIDS.
Women infected with HIV can pass the virus to the fetus during pregnancy and childbirth. The infected woman can also pass the virus to the child who is breastfeeding through breastfeeding.
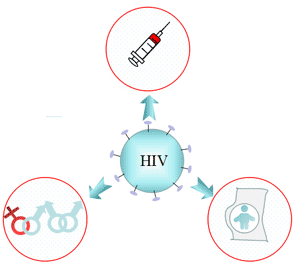
Figure 6 Transmission of AIDS
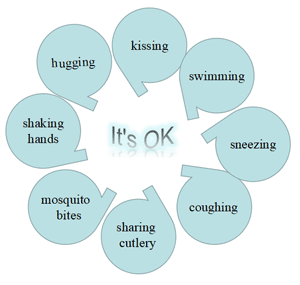
Figure 7 No HIV transmission
It is well known that AIDS is an Immunodeficiency disease caused by the Human Immunodeficiency Virus (HIV). HIV selectively invades CD4 molecules, mainly T4 lymphocytes, monocyte macrophages, dendritic cells, and the like.
The CD4 molecule on the cell surface is the HIV receptor. After the HIV membrane protein gp120 binds to the CD4 on the cell membrane. The conformation of gp120 changes, causing gp41 to be exposed. Meanwhile, gp120-CD4 binds to the chemokines CXCR4 or CXCR5 on the surface of the target cells to form the cd4-gp120-cxcr4 /CXCR5 tri-molecular complex. Gp41 uses its hydrophobic properties to mediate the fusion of viral cysts and cell membranes. Eventually the cells are destroyed. Over time, HIV destroys so many of these cells that the body cannot fight infection and disease, making people more susceptible to other infections or infection-related cancers.
The three stages of HIV infection are: Acute HIV Infection Stage; Clinical Latency Stage; AIDS (Acquired Immunodeficiency Syndrome).
Many (but not all) people develop flu-like symptoms within 2 to 4 weeks of infection. HIV symptoms include fever, gland swelling, sore throat, AIDS rash, muscle and joint pain, and headache in this stage.
The incubation period refers to the period in which the virus survives or develops in the human body without causing symptoms. During the clinical latency stage, standard laboratory tests fail to detect the virus. But people in this period can still transmit HIV to others. The average clinical latency stage was 10 years.
AIDS is the most severe stage of HIV infection. The immune system of AIDS patients is seriously damaged, and they will suffer from more and more serious diseases, called opportunistic infections. When your CD4 cell count is less than 200 cells per cubic millimeter of blood (200 cells/mm3), you are considered to have developed AIDS. (In populations with a healthy immune system, the number of CD4 cells is between 500 and 1600/mm3).
Primary HIV-related nervous system diseases include Peripheral neuropathy, myelopathy and HIV encephalopathy. As these diseases are related to clinical dementia, they are called AIDS dementia complex (ADC). HIV-associated dementia (HAD) often has low memory, inattention, unresponsiveness, and time and space orientation disorders as initial symptoms, and the disease progresses progressively. Patients with advanced HAD can develop severe dementia [11].
HIV wasting syndrome showed a significant decrease in body weight (> 10%) and chronic diarrhea or weakness. Intermittent or persistent fever is also one of the basis for HIV diagnosis.
Kidney damage caused by HIV includes thrombotic microangiopathy caused directly by HIV, and immune-mediated glomerulonephritis and nephropathy. HIV-induced kidney disease was first reported by American scholar Rao in 1984 and officially named HIV associated Nephropathy (HIVAN). Renal biopsy is the primary means of confirming HIVA.
At present, all countries in the world have included HIV in blood screening criteria. The methods used for screening mainly include HIV antibody detection, HIV antigen-antibody detection, and HIV nucleic acid detection [12].
HIV antibodies in serum are an indirect indicator of HIV infection. The widely used methods of AIDS test are the fourth generation test, enzyme-linked immunosorbant assay and chemiluminescent immunoassay. The window period of AIDS can be shortened to 14 ~ 21 days [13]. Although HIV antibodies were not detected during the window period, they were contagious. Other test methods include: particle agglutination reagent, Dot-blot assay (a rapid ELISA method.)
Pathogen detection mainly refers to direct detection of virus or viral genes from host samples by virus isolation and culture, electron microscopic observation, viral antigen detection and gene assay. For clinical diagnosis, antigen detection and RT-PCR (reverse transcription-PCR) are generally used.
HIV nucleic acid test can be used for the auxiliary diagnosis, course monitoring, treatment program guidance, determination of curative effect and prediction of disease progression, etc.
Commonly used methods for detecting HIV viral load include reverse transcription PCR (RT-PCR), nucleic acid sequence based amplification (NASBA), branched DNA hybridization (bDNA), real-time fluorescence quantitative PCR.
There is currently no effective HIV treatment, but with proper medical care, HIV can be controlled. For example, Magic Johnson was diagnosed with the HIV virus in 1991. After years of adherence to treatment, in March 1997, after examination, the doctor determined that Johnson had overcome the virus and fully recovered.
If you are HIV-negative, you have several options to protect yourself from HIV infection. The more you take these actions, the safer you will be.
If you are HIV+, you can take many steps to prevent HIV transmission to HIV-negative partners.
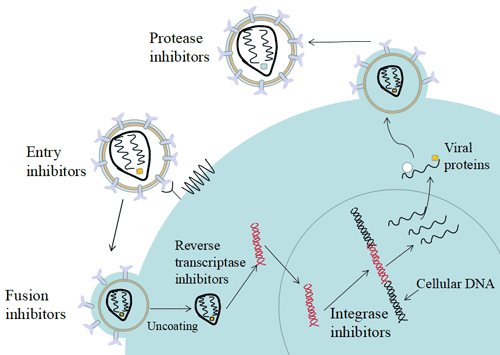
Figure 8 Life cycle of HIV and targets of anti-HIV drug
Based on the life cycle of HIV-1 as described above, the anti-aids drugs currently in use or under development mainly include:
At present, the world's hottest and most successful new anti-aids drugs with new mechanism of action mainly focus on the two fields of HIV-1 entry inhibitor and HIV-1 integrase inhibitor [20]. This new anti-AIDS drug has brought new therapeutic hopes to more and more drug-resistant patients [21].
In May 2018, a research team used CRISPR/Cas9 editing technology to develop an effective method to destroy the regulatory genes of HIV and successfully inhibit the proliferation of HIV-1 in infected cells [22].
There are currently no HIV vaccine to prevent or treat HIV infection. However, scientists are working hard to develop. Currently, a vaccine trial called HVTN702, supported by the National Institutes of Health, is testing whether an experimental vaccine program can safely prevent HIV infection among adults in South Africa.
References
[1] Barrésinoussi F, Chermann J C, Rey F, et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS) [J]. Science, 1983, 220(4599):868-871.
[2] Gallo RC, Sarin PS, Gelmann EP, et al. Isolation of human T-cell leukemia virus in acquired immune deficiency syndrome (AIDS) [J]. Science, 1983, 220(4599):865-867.
[3]Ratner L, Haseltine W, Patarca R, et al. Complete nucleotide sequence of the AIDS virus, HTLV-III [J]. Nature, 1985, 313(6000):277-284.
[4]Sanchez-Pescador R, Power M D, Barr P J, et al. Nucleotide sequence and expression of an AIDS-associated retrovirus (ARV-2) [J]. Science, 1985, 227(4686):484.
[5]Wain-Hobson S, Sonigo P, Danos O, et al. Nucleotide sequence of the AIDS virus, LAV [J]. Cell, 1985, 40(1):9-17.
[6]Sharp P M, Hahn B H. Origins of HIV and the AIDS Pandemic [J]. Cold Spring Harbor Perspectives in Medicine, 2011, 1(1):a006841.
[7]Rhodes T, Singer M, Bourgois P, et al. The social structural production of HIV risk among injecting drug users [J]. Social Science & Medicine, 2005, 61(5):1026-1044.
[8] Smith J H, Whiteside A. The history of AIDS exceptionalism [J]. Journal of the International Aids Society, 2010, 13(1):1-8.
[9] Votteler J, Schubert U. Human Immunodeficiency Viruses: Molecular Biology [J]. Encyclopedia of Virology, 2008, 511:517-525.
[10] Hollingsworth TD, Anderson RM, Fraser C. HIV-1 transmission, by stage of infection [J]. The Journal of Infectious Diseases, 2008, 198(5):687-693.
[11]Moore D J, Masliah E, Rippeth J D, et al. Cortical and subcortical neurodegeneration is associated with HIV neurocognitive impairment [J]. Aids, 2006, 20(6):879-887.
[12]Patel, P, Mackellar, D, Simmons, P, et al. Detecting acute human immunodeficiency virus infection using 3 different screening immunoassays and nucleic acid amplification testing for human immunodeficiency virus RNA, 2006-2008 [J]. Archives of Internal Medicine, 2010, 170(1):66-74.
[13] Petak F, Albu G, Lele E, et al. Cost-effectiveness of a Fourth-Generation Combination Immunoassay for Human Immunodeficiency Virus (HIV) Antibody and p24 Antigen for the Detection of HIV Infections in the United States [J]. HIV Clinical Trials, 2012, 13(1):11-22.
[14] Schröder A R W, Shinn P, Chen H, et al. HIV-1 Integration in the Human Genome Favors Active Genes and Local Hotspots [J]. Cell, 2002, 110(4):521-529.
[15] Tomkowicz B, Collman R G. HIV-1 entry inhibitors: closing the front door [J]. Expert Opin Ther Targets, 2004, 8(2):65-78.
[16] Young S D. Inhibition of HIV-1 integrase by small molecules: the potential for a new class of AIDS chemotherapeutics [J]. Curr Opin Drug Discov Devel, 2001, 4(4):402-410.
[17] Reeves D J D, Piefer A J. Emerging Drug Targets for Antiretroviral Therapy [J]. Drugs, 2005, 65(13):1747-1766.
[18] Temesgen Z, Feinberg J E. Drug evaluation: bevirimat--HIV Gag protein and viral maturation inhibitor [J]. Current Opinion in Investigational Drugs, 2006, 7(8):759.
[19] Li F, Goila-Gaur R, Salzwedel K, et al. PA-457: A Potent HIV Inhibitor That Disrupts Core Condensation by Targeting a Late Step in Gag Processing [J]. Proceedings of the National Academy of Sciences of the United States of America, 2003, 100(23):13555-13560.
[20]Opar A. New HIV drug classes on the horizon [J]. Nature Reviews Drug Discovery, 2007, 6(4):258.
[21] Moore J P, Stevenson M. New targets for inhibitors of HIV-1 replication [J]. Nature Reviews Molecular Cell Biology, 2000, 1(1):40.
[22] Ophinni Y, Inoue M, Kotaki T, et al. CRISPR/Cas9 system targeting regulatory genes of HIV-1 inhibits viral replication in infected T-cell cultures [J]. Scientific Reports, 2018, 8.


Comments
Leave a Comment