Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
Immunohistochemistry (IHC) is a commonly detection technique in clinical pathological diagnosis. Since the 1970s, immunohistochemical technology has been applied to pathological diagnosis, which has a huge impact on the diagnosis of tumors, tumor classification, and prognosis. It has also expanded people's understanding of various diseases and tumor formation processes, and improved The level of pathological diagnosis and research. This article focuses on the clinical application of immunohistochemistry and the clinical significance of common immunohistochemical indicators.
2. What is Pathological Diagnosis?
3. The Appliction of IHC in Pathological Diagnosis?
Immunohistochemistry (IHC) is the application of the basic principles of immunology-the antigen-antibody reaction, that is, the binding between the antibody and the antigen is highly specific. First, a certain chemical substance in the tissue or cell is extracted as an antigen or semi-antigen. Specific antibodies are then obtained by immunizing the animals, and the antibodies are used to detect similar antigenic substances in tissues or cells. Because the complex of antigen and antibody is colorless, it is necessary to display the site where the antigen and antibody bind by means of histochemical methods (fluorescein, enzyme, metal ion, isotope) in order to achieve unknown antigens are studied qualitatively, locally or quantitatively (Figure 1).
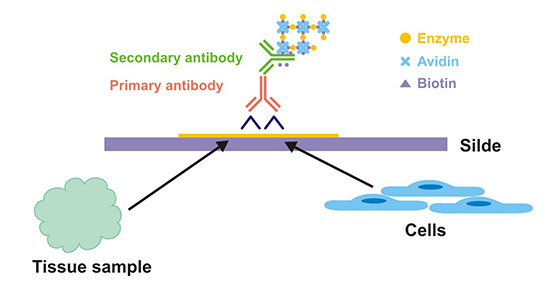
Figure 1. The theoretical diagram of IHC
The samples of immunohistochemistry are mainly tissues. The tissue is from a patient or animal and is frozen or embedded in paraffin. These tissues were made into sections with a thickness of about 4 μm and processed after sealing. If the sample is a cell, it is often called Immunocytochemistry (ICC). For ICC, most of the extracellular matrix are removed, leaving only whole cells for staining. ICC sources can be cell suspensions, from patients or animals (such as blood smears, swabs, etc.), or tissue culture cell lines performed in the laboratory.
Pathological diagnosis is to study the morphological structure and functional metabolism during the occurrence and development of disease, and to provide the necessary theoretical and practical basis for disease diagnosis, treatment and prevention. Pathological diagnosis is to perform fixed staining on tumor specimens from surgery or autopsy, and then perform histological examination under a microscope in order to diagnose the disease. The samples are more from living people.
Despite the rapid development of various imaging techniques, pathological diagnosis is still the most reliable of various tumor examination methods. Pathological diagnosis is known as the "gold standard" and is the final diagnosis of disease. If the pathological diagnosis is compared with the test diagnosis such as biochemical immunity, the pathological diagnosis is like the actual evidence such as fingerprints, footprints, and DNA obtained by the police. Because it observes the cell morphology and structure of suspected diseased tissue through a microscope, it can directly see what kind of pathological changes occur in the tissue, and can make a more accurate judgment of the disease, especially in the diagnosis of tumor properties.
Currently, the application of immunohistochemical technology in clinic includes the following eight aspects:
However, with the widespread application of IHC, it has been found that there are some limitations in immunohistochemistry. The limitations of IHC in tumor diagnosis are mainly antibody specificity and interpretation. There must be positive and negative controls during the immunohistochemical operation. As a technical integrity quality control, if the control group is ignored or not ideal, the results of immunohistochemical staining should be treated with caution.
The correct results of immunohistochemistry not only rely on standardized operations in technical steps, but also depend on correct interpretation. When reporting the results of immunohistochemical staining, they should not be interpreted in isolation. The diagnosis and differential diagnosis, and the characteristics of the antibodies used should be considered, as well as the nature of the tissue under study. At the same time, the interference of false positive and false negative results should be paid attention to. In-depth research on the principles and techniques of IHC, we must be familiar with the true positive reaction sites of various antibodies, realize the standardization of immunohistochemistry among laboratories, and make immunohistochemistry play the biggest auxiliary role in pathological diagnosis.
False positives are incorrect positioning of positive signals, including uneven coloring, background coloring, and edge effects. In addition, certain specific components of the tissue can also cause false positive results. False negative in immunohistochemical results means that all antibody-labeled sections are negative and there is no positive signal. False negative results are not true reactions.
Everyone knows that pathological examination is the gold standard for clinical diagnosis and treatment, especially for cancer patients. The results of IHC are particularly important for the diagnosis and treatment of tumors and prognostic analysis. This article summarizes the current series of inspections and their significance.
Current research shows that the recurrence and metastasis of most tumors depend on Ki-67 and p53 values, not on the type of tumor tissue tissue. Such as moderately differentiated adenocarcinoma, if Ki-67 and p53 values exceed 50%, the prognosis is poor. In contrast, if the tumor is typed as poorly differentiated adenocarcinoma, and the Ki-67 and p53 values are lower, the prognosis will be slightly better than that of moderately differentiated or highly differentiated cancer.
P-glycoprotein (P-gp): it acts as a drug pump and locates on membrane and cytoplasm. If the positive rate is higher, the resistance to drugs (doxorubicin, daunorubicin, epirubicin , Mitoxantrone, vinblastine, vincristine, paclitaxel, and taxol) is stronger:
Glutathione S-transferase (GST π): it plays a key role in detoxification and mainly locates on cytoplasm.. The positive rate is higher, the resistance to drugs (doxorubicin, cisplatin, nitrogen mustard, cyclophosphamide and tumor cells rather) is stronger.
Topoisomerase II (TOPOⅡ): it acts as a target to drugs and mainly locates on nucleus. the higher the positive rate, the more effective the following drugs: anthracycline antibiotics and podophyllotoxins, such as VP-16, teniposide, Ellipticine, neomycin, daunorubicin, epirubicin, doxorubicin, VM26. Those with a high positive rate are particularly effective against VP-16.
Ki-67 is the marker of cell proliferation and mainly locates on nucleus. The positive rate is higher, the tumor proliferation is faster, and the degree of malignancy is higher .
The prognosis markers of breast cancer resistance include P-gp, GSTπ, TOPOⅡ, Ki-67, ER, PR, and HER2.
The estrogen receptor (ER) mainly functions as a sex hormone and locates on nucleus. The higher positive rate, the more effective the tumor is for endocrine therapy and the better the prognosis.
The progesterone receptor (PR) mainly functions as a sex hormone and locates on nucleus. The higher the positive rate, the more effective the tumor is for endocrine therapy and the better the prognosis.
The C-erbB-2 (HER2) gene mainly functions as oncogene product and locates on cytoplasm. The higher positive rate, the higher the malignancy of the tumor.
p53, a tumor suppressor gene, is divided into wild type (Wtp53) and mutant (Mtp53). Wtp53 is difficult to detect due to micro-immunohistochemistry. Mtp53 can be determined by IHC. After mutation, it loses the ability of initiating apoptosis. High expression of mutant p53 indicates that the cell has high proliferation, poor differentiation, higher degree of malignancy, and poor prognosis.
95% of GIST characteristically expresses CD117.
GIST characteristically expresses DOG1, and DOG1 positive expression sites are similar to CD117. Note that DOG1 can be expressed in some CD117-negative GISTs (6%). DOG1 is highly expressed in cases of gastric GIST, epithelioid GIST, and PDGFRA mutations. Most GIST expresses CD34 (70%), focally expresses SMA (40%), S-100 (5%), and usually does not express desmin (2%).
The latest WHO subtype of lymphoma has 33 subtypes, and the prognosis and treatment of each subtype are different. The diagnosis and typing of lymphoma is extremely difficult, which is the difficulty in pathology. The immunohistochemical scheme for the diagnosis of lymphoma must be a "dual package", that is, each tissue must be labeled with more than two antibodies.
The diagnosis of B-cell lymphoma must be positively confirmed by CD20 and CD79a positive, and also confirmed by CD3 negative. Therefore, the diagnosis of lymphoma requires about 8-10 antibodies to accurately reflect the various subtypes of lymphoma. information.


Comments
Leave a Comment