Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
Cardiac muscle, like skeletal muscle, appears striated due to the organization of muscle tissue into sarcomeres. While similar to skeletal muscle, cardiac muscle is different in a few ways. Cardiac muscles are composed of tubular cardiomyocytes, or cardiac muscle cells. The cardiomyocytes are composed of tubular myofibrils, which are repeating sections of sarcomeres. Intercalated disks transmit electrical action potentials between sarcomeres.
The heart is mainly composed of cardiac muscle, and this muscle plays a critical role in the function of the heart. Note that our heartbeats are an outcome of the constant contraction of the cardiac muscle. As long as this muscle gets a sufficient supply of oxygen and nutrients, it will never cease its contracting process.
No organism can sustain alive without the function of the cardiac muscle. The cardiac muscle facilitates the pumping action of the ventricle. It squeezes blood out of your heart while contracting, and retrieves blood by relaxing. It pumps the deoxygenated blood from the right atrium and right ventricle to the lungs, and pumps oxygenated blood through the left atrium and left ventricle to other parts of the body and the aorta.
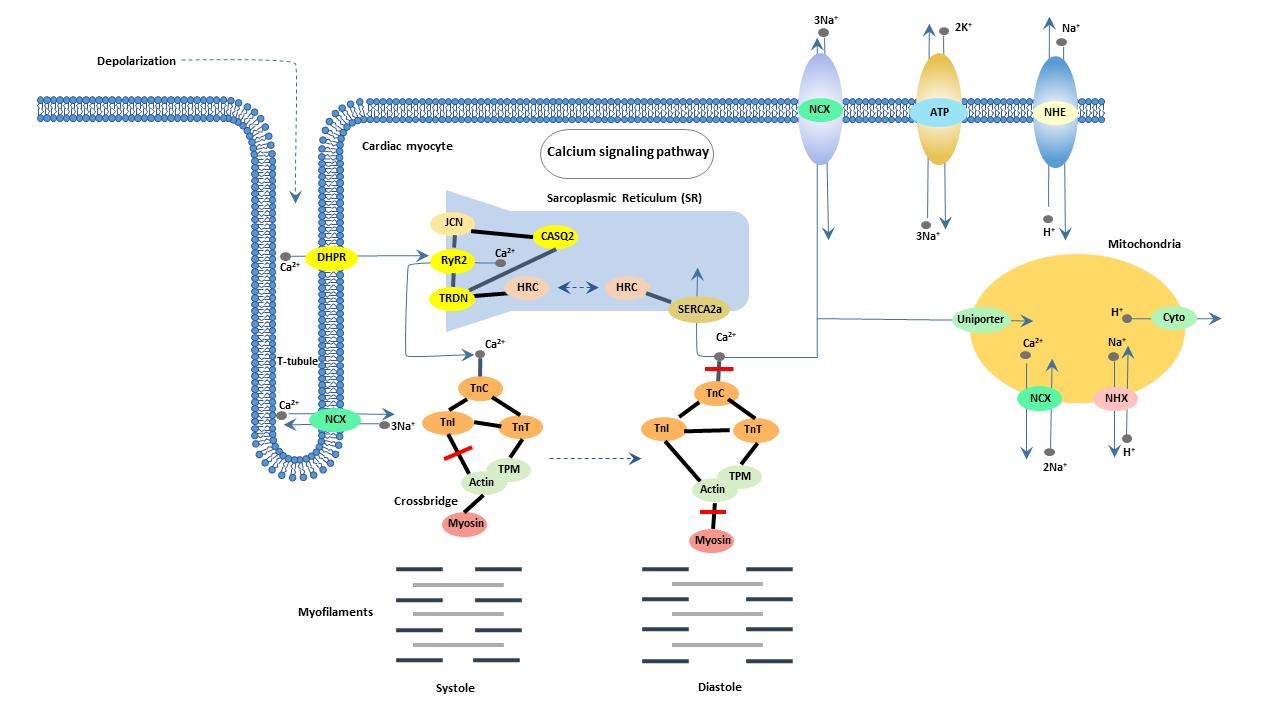
Contraction of the heart is a complex process initiated by the electrical excitation of cardiac myocytes. In cardiac myocytes, Ca2+ influx induced by activation of voltage-dependent L-type Ca2+ channels (DHP receptors) upon membrane depolarization triggers the release of Ca2+ by Ca2+ release channels (ryanodine receptors) of sarcoplasmic reticulum (SR) through a Ca2+ -induced Ca release (CICR) mechanism. Ca>2+ ions released by the CICR mechanism diffuse through the cytosolic space to contractile proteins to bind to troponinC resulting in the release of inhibition induced by troponinI.
Thereby, the Ca2+ binding to troponinC triggers the sliding of thin and thick filaments, that is, the activation of a crossbridge and subsequent cardiac force development and cell shortening.

