Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
TGF-β is a growth factor with multi-function on target cells. Almost every cell in the body produces TGF-β and has its receptor. It plays an important regulatory role in the differentiation of tissues and cells, and can stimulate or inhibit the proliferation of various cells. In addition, it has a significant impact on the body's immune system. They play an important role in tumorigenesis and metastasis.
In tumor cells, the role of TGF-β family is to regulate the balance between self-repair and differentiation of cancer stem cells (CSCs). It has dual effects on tumor cells. TGF-β signaling switches from a tumor suppressor to a tumor promoter are shown.
A good role: TGF-β protects against autoimmune intestinal diseases; TGF-β is often used as a tumor suppressor due to its strong anti-proliferation effect; by stimulating the synthesis of matrix proteins and reducing matrix degradation, TGF-β has a unique effect on extracellular matrix and promotes wound healing; In an infection, it prevents collateral damage from the immune system; TGF-β is usually an active inhibitor of inflammation; TGF-β can inhibit the proliferation of T lymphocytes, B lymphocytes, monocytes and macrophages. TGF-β may play a role in preventing depression.
A bad role: TGF-β can cause local inflammation and inhibits the formation of acetylcholine; In an inflammatory environment, TGF-β produces pro-inflammatory cells, once cells become resistant to drugs, TGF-β mainly supports tumor growth and metastasis by promoting immune escape and angiogenesis; TGF-β decreases slow-wave sleep and reduces muscle regeneration; TGF-β promotes tumor proliferation. The increased TGF-β level was significantly correlated with lymph node metastasis and poor prognosis in gastric cancer patients; TGF-β reduces the effect of vitamin D receptor; TGF-β has both positive and negative effects on bone mineral density. Scientists believe that in the short term, it can increase bone mineral density, but in the long term, TGF-β can reduce bone mineral density; TGF-β is elevated in the blood of patients with aggressive prostate cancer.
Colorectal cancer: It is one of the most common fatal malignancies worldwide. It develops in about 5 percent of the adult population in the United States, and nearly half of them will die from the disease [1]. Furthermore, inactivation of the Smad3 gene, a downstream signaling molecule of the TGF-β receptor, may lead to the development of neoplastic lesions in the murine colon. TGF-β inhibit tumor progression in colon cancer by inhibiting IL-6 signal transmission [2]. Colorectal cancer cells with the functions of autocrine TGF-β 1, TGF-β 1 indirectly promotes tumor angiogenesis by up-regulating the expression of vascular endothelial growth factor (VEGF). This may be one of the mechanisms by which TGF-β 1 promotes proliferation, infiltration and metastasis of colorectal cancer cells.
The tumor of the hematopoietic system: In tumor diseases of hematopoietic system, the destruction of TGF-β signaling pathway leads to the tolerance of cells to TGF-β and escape the growth inhibition effect of TGF-β.
Papillary thyroid carcinoma: In papillary thyroid carcinoma, the expressions of TGF-β 1, non-metastasis (nm23-H1) and cell adhesion molecule (CD31) are related to the metastasis and pathological staging of papillary thyroid carcinoma. TGF-β 1, CD31 and microvascular density (MVD) expression gradually increased, nm23-H1 expression gradually decreased, which are important signals of the disease progression and tumor metastasis of papillary thyroid carcinoma. The expression levels of TGF-β 1, nm23-H1 and CD31 in papillary thyroid carcinoma can be used as one of the indicators to determine disease progression and tumor metastasis. In addition, mutations in the components of the TGF-β pathway can lead to inherited cancer and developmental disorders [3].
TGF-β is involved in a wide range of regulatory effects and is important for maintaining tissue homeostasis. Abnormal expression of TGF-β may lead to a series of diseases and cancer. Research results in recent years have confirmed that TGF-β and its receptor are closely related to the occurrence and development of tumors.
TGF-β 1 is the most important member of the TGF-β family. High expression of TGF-β 1 can be observed in most tumors. It has been confirmed that high level of TGF-β 1 is expressed in various tumor tissues, including gastric cancer, colorectal cancer and colon cancer [4][5][6].
Inhibition effect of TGF-β on tumor: In normal cells, TGF-β inhibits cell proliferation, induces differentiation or induces apoptosis by blocking cells from G1 into S phase. Therefore, in the early stage of tumorigenesis, TGF-β can block the growth cycle and act as a tumor suppressant to prevent the proliferation of tumor cells.
Promotion effect of TGF-β on tumor: In the late stage of tumor development, TGF-β are beneficial to tumor cell growth and metastasis. TGF-β promotes tumor invasion and metastasis mainly through three aspects:
(I) TGF-β promotes metastasis of tumor cells: recent studies have revealed that TGF-β plays an important role in the metastasis of breast cancer and prostate cancer bone. In the development of breast cancer, TGF-β switches from tumor inhibition to metastasis promoting factor [7].
(II) TGF-β promotes the immune escape of tumor cells. TGF-β secreted by tumor cells can help tumor cells to evade the host immune system monitoring and facilitate the process of invasion and metastasis. It is known that TGF-β can up-regulate the activity of urokinase and its receptor, promote breast cancer metastasis and enhance the invasiveness of human pancreatic cancer cells. This effect can be blocked by anti-TGF-β antibodies [8]. TGF-β can also act directly on lymphocytes and play an important role in tumor evasive immune surveillance [9].
(III) TGF-β promotes angiogenesis. TGF-β signal promotes tumor angiogenesis by enhancing the pericyte-endothelium association [10]. TGF-β promotes angiogenesis induced by tumor and plays an important role in bone metastasis of prostate cancer. TGF-β was found to be closely related to primary invasion and secondary metastasis of tumor cells in multiple tumors including colon cancer, liver cancer and breast cancer [11]. In addition, Hsu S et al found that in the undifferentiated colorectal cancer cell line U9, TGF-β 1 not only directly induces tumor cell proliferation, but also stimulates tumor cell invasion and metastasis [12]. Guzinska et al [13] also have similar reports.
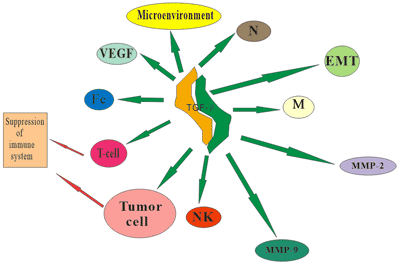
Figure 1. TGF-β promotes the invasion and metastasis of tumor cells
M: Macrophages; N: Neutrophil; NK: Natural killer cells; Fc: Fiber cells; VEGF: Vascular endothelial growth factor; EMT: Epithelial-mesenchymal transition; MMP-2, MMP-9: Metal matrix proteinase-2, Metal matrix proteinase-9.
TGF-β signals through the type II receptor mediate growth inhibition of carcinoma cells. When TβRII is deleted or downregulated, the result is increased chemokine/chemokine-receptor signaling, such as CXCL1-CXCL5/CXCR2 and SDF-1-CXCR4. Host-derived immature myeloid Gr-1+CD11b+cells are recruited into the tumor microenvironment through these chemokine mechanisms. These Gr-1+CD11b+cells express high level of MMPs and TGF-β 1, which promote tumor invasion and immune suppression. The effect of Gr-1+CD11b+cells on the tumor microenvironment and host immune surveillance constitute a tumor-promoting mechanism of TGF-β signaling. The gene mutation in TGF-β signaling pathway leads to the cell's tolerance to TGF-β, which inactivates the senescence and apoptosis pathways. Eventually cell carcinogenesis may occur.
Ligand and tumor: BMPs has two effects on tumor cells, on the one hand, it can inhibit tumor proliferation[14]. On the other hand, BMPs has an anti-apoptotic effect [15].
TGF-β signaling transduction is dependent on the receptor TβRⅠand TβR II, receptor mutation will lead to a tolerance of TGF-β cells. The deactivation of II receptor has been reported in gastric cancer, breast cancer and small cell lung cancer cell lines. Homologous deletion of genes TβRⅠ exist in human pancreatic cancer and cholangiocarcinoma [16].
R-smad plays a key role in connecting signaling pathways, and the R-smad mutation is associated with cancer. Smad-2 gene mutation occurs in a small part of colorectal cancer [17]. Loss of Smad-3 expression has been noted in gastric cancer and T cell lymphoblastic leukemia [18], mutation or expression loss of Smad-2 and Smad-4 is associated with the development of multiple tumors, such as pancreatic, colorectal, lung and skin cancer.
With growing clinical evidence that TGF-β acts as a tumor-derived immunosuppressor, an inducer of tumor mitogens, a promoter of carcinoma invasion, and a trigger of prometastatic cytokine secretion, there is growing interest in TGF-β as a therapeutic target.
Prevention: In early stage of cancer, TGF-β appears as a tumor suppressor factor. Therefore, the application of TGF-β inducer may prevent tumorigenesis in patients with high tumor incidence. Clinical application of effective chemical preventive drugs: Anti-estrogen drug tamoxifen.
Treatment: Different tumors have different treatment methods. In the case of breast cancer, since most tumor cells are resistant to TGF-β, the treatment strategy is to inactivate TGF-β or to restore the responsiveness of tumor cells to TGF-β. TGF-β 1 inhibitor may be a treatment for breast cancer, which mainly including TGF-β 1 antibody, TGF-β 1 binding protein, or antisense TGF-β mRNA. Nogginis, a BMPs antagonist, which acting on pituitary prolactin tumor, can significantly inhibit the tumorigenicity of tumor cells [19]. The polypeptide or peptide drug simulate the smad4-related transcription complex, which may activate downstream signaling pathways and inhibit tumor cell proliferation. In addition, since the TGF-β signaling has the function of tumor suppressor and tumor promotion, it is difficult to target this pathway for tumor treatment [20].
Tumor markers(TM) refer to the following substances: Substances produced by malignant tumor cells; Substances produced by the host in response to a tumor.
Ideal tumor marker:
Macrophage inhibitory cytokine-1(MIC-1, GDF15) is an important member of the TGF-β superfamily. As a tumor marker, MIC-1 has certain application in the early diagnosis of pancreatic cancer. Levels of MIC-1 also increased in the serum of patients with the same symptoms as pancreatic cancer, such as cholangiocarcinoma and ampulla carcinoma [21][22][23].
TGF-β is also has been recently considered as a possible liver tumour marker. In the diagnosis of HCC induced by HBV(hepatitis B virus), TGF-β 1 and TGF-β 1 mRNA were shown to be sensitive indicators. As a tumor marker, TGF-β 1 can be used in many diseases, TGF-β 1 can be used as a non-specific tumor marker for nasopharyngeal carcinoma, which is of great significance in guiding clinical staging and determining curative effect and prognosis. TGF-β 1 is related to the pathogenesis of NSCLC (non-small-cell lung cancer), and the serum TGF-β 1 level can be used as one of the important tumor markers for the auxiliary diagnosis and disease observation of NSCLC patients. TGF-β is one of the tumor markers of primary liver cancer. In gastric cancer and prostate cancer, TGF-β also be a potential tumor marker. In addition to acting as a tumor marker, TGF-β family also regulates some tumor markers.
In general, you want TGF-β to be in balance, not too high or too low. So you need to know how to suppress or increase it in a natural way.
In the case of intestinal diseases, how can we increase the TGF-β in the gut?
Ingestion of TGF-β themselves: Both colostrum and breast milk contain TGF-β;
Insulin-like growth factor: colostrum and pilose antler;
Curcumin, retinol;
Probiotics, lactobacillus;
Vitamin D3 (active form)-increases blood TGF-β;
Alkannin-increased intestinal TGF-β;
Vascular endothelial growth factor-increases TGF-β in the gut.
References
[1] Weir H K, Thun M J, Hankey B F, et al. Annual report to the nation on the status of cancer, 1975-2000, featuring the uses of surveillance data for cancer prevention and control [J]. Journal of the National Cancer Institute, 2003, 95(17): 1276.
[2] Becker C, Fantini M C, Schramm C, et al. TGF-β Suppresses Tumor Progression in Colon Cancer by Inhibition of IL-6-Signaling [J]. Zeitschrift Für Gastroenterologie, 2004, 21(4): 491-501.
[3] Waite K A, Eng C. From developmental disorder to heritable cancer: it's all in the BMP/TGF-β family [J]. Nature Reviews Genetics, 2003, 4(10): 763-73.
[4] Kinugasa S, Abe S, Tachibana M, et al. Overexpression of Transforming Growth Factor-β1 in Scirrhous Carcinoma of the Stomach Correlates with Decreased Survival[J]. Oncology, 1998, 55(6): 582-587.
[5] Friedman E, Gold L I, Klimstra D, et al. High levels of transforming growth factor beta 1 correlate with disease progression in human colon cancer [J]. Cancer Epidemiol Biomarkers Prev, 1995, 4(5): 549.
[6] Shim K S, Kim K H, Han W S, et al. Elevated serum levels of transforming growth factor-beta1 in patients with colorectal carcinoma: its association with tumor progression and its significant decrease after curative surgical resection [J]. Cancer, 1999, 85(3): 554-561.
[7] Tang B, Vu M, Booker T, et al. TGF-β switches from tumor suppressor to prometastatic factor in a model of breast cancer progression[J]. Journal of Clinical Investigation, 2003, 112(7): 1116.
[8] Albo D, Berger D H, Tuszynski G P. The Effect of Thrombospondin-1 and TGF-β 1 on Pancreatic Cancer Cell Invasion [J]. Journal of Surgical Research, 1998, 76(1): 86-90.
[9] Thomas D A, Massagué J. TGF-β directly targets cytotoxic T cell functions during tumor evasion of immune surveillance [J]. Cancer Cell, 2005, 8(5): 369-380.
[10] Zonneville J, Safina A, Truskinovsky A M, et al. TGF-β signaling promotes tumor vasculature by enhancing the pericyte-endothelium association [J]. Bmc Cancer, 2018, 18(1): 670.
[11] Yap A S, Crampton M S, Hardin J. Making and breaking contacts: the cellular biology of cadherin regulation [J]. Current Opinion in Cell Biology, 2007, 19(5): 508-514.
[12] Hsu S, Huang F, Friedman E. Platelet-derived growth factor-β increases colon cancer cell growth in vivo by a paracrine effect [J]. Journal of Cellular Physiology, 1995, 165(2): 239-245.
[13] Guzinska-Ustymowicz K, Kemona A. Transforming growth factor beta can be a parameter of aggressiveness of pT1 colorectal cancer [J]. World Journal of Gastroenterology, 2005, 11(8): 1193.
[14] Buckley S, Shi W, Driscoll B, et al. BMP4 signaling induces senescence and modulates the oncogenic phenotype of A549 lung adenocarcinoma cells [J]. American Journal of Physiology Lung Cellular & Molecular Physiology, 2004, 286(1): 81-6.
[15] Kim J S, Crooks H, Dracheva T, et al. Oncogenic β-Catenin Is Required for Bone Morphogenetic Protein 4 Expression in Human Cancer Cells [J]. Cancer Research, 2002, 62(10): 2744-2748.
[16] Goggins M, Shekher M, Turnacioglu K, et al. Genetic alterations of the transforming growth factor beta receptor genes in pancreatic and biliary adenocarcinomas [J]. Cancer Research, 1998, 58(23): 5329-5332.
[17] Sjoblom T, Jones S, Wood L D, et al. The Consensus Coding Sequences of Human Breast and Colorectal Cancers [J]. Science, 2006, 314(5797): 268-74.
[18] Levy L, Hill C S. Alterations in components of the TGF-beta superfamily signaling pathways in human cancer [J]. Cytokine & Growth Factor Reviews, 2006, 17(1): 41-58.
[19] Paezpereda M, Giacomini D, Refojo D, et al. Involvement of bone morphogenetic protein 4 (BMP-4) in pituitary prolactinoma pathogenesis through a Smad/estrogen receptor crosstalk [J]. Proc Natl Acad Sci USA, 2003, 100(3): 1034-1039.
[20] Hawinkels L J, Ten P D. Exploring anti-TGF-β therapies in cancer and fibrosis [J]. Growth Factors, 2011, 29(4): 140-152.
[21] Koopmann J, Buckhaults P, Brown D A, et al. Serum macrophage inhibitory cytokine 1 as a marker of pancreatic and other periampullary cancers.[J]. Clinical Cancer Research, 2004, 10(7): 2386-2392.
[22] Koopmann J, Rosenzweig C N, Zhang Z, et al. Serum markers in patients with resectable pancreatic adenocarcinoma: macrophage inhibitory cytokine 1 versus CA19-9.[J]. Clinical Cancer Research, 2006, 12(2): 442-446.
[23] Liang J J, Kimchi E T, Staveley-O'Carroll K F, et al. Diagnostic and Prognostic Biomarkers in Pancreatic Carcinoma [J]. International Journal of Clinical & Experimental Pathology, 2009, 2(1): 1-10.


Comments
Leave a Comment