Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
As mentioned in the article entitled "G protein-Coupled Receptor - Targets for Drug Therapy", GPCRs is an important drug target, and currently about 40% of the marketed drugs are designed based on GPCRs. About 34% of drug targets approved by the food and drug administration (FDA) are members of this family. There are about 370 GPCRs that can become drug targets. Currently, statistics from GproteinDb (The G protein database) have reported that a total of 476 GPCR drugs approved by the FDA includes 92% small molecule drugs, 5% polypeptide drugs, 2% are protein drugs. As the Figure 1 shows, the drugs targeting GPCR and approved are mainly small molecule drugs, and the anti-GPCR antibody drugs are mostly in trial. So why are there so few anti-GPCR antibody drugs? And how are the anti-GPCR antibody drugs currently under development?
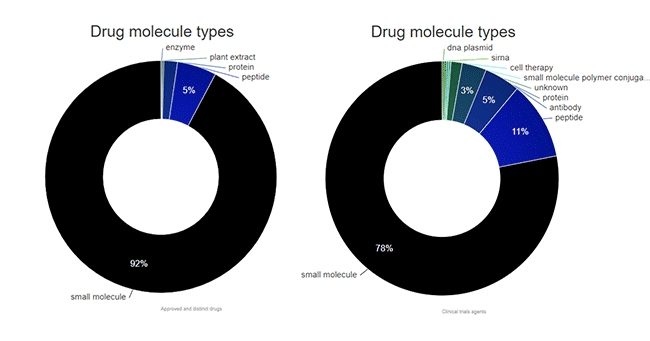
Figure 1. The types of targeting-GPCR drugs approved by FDA and in trail
1. Why are There So Few Anti-GPCR Antibody Drugs?
2. The Latest Progress of Anti-GPCR Antibody Drugs
The fundamental reason for the lack of antibody drugs targeting GPCRs is the difficulty of development. First, the preparation of GPCR antigens is difficult (CUSABIO three technology platforms fuel transmembrane proteins development: virus like particles (VLPs), detergent micelle and nanodisc platforms). Secondly, GPCR antibody screening methods also need to be designed according to specific targets, and cannot be simply screened on the basis of affinity. In addition, the method for functional identification of GPCR antibodies is not perfect. In recent years, with the development of transmembrane protein expression technology, the continuous deepening of GPCR structure and function research and the continuous maturity of GPCR antibody screening methods, more and more GPCR drug research and development are trying to use protein antibodies.
The types of developed and developing targeting-GPCR antibody drugs include naked antibodies, bispecific antibodies, ADCs, nanobodies, and CAR-T. GPCR antibodies are also being investigated as combination therapy. The GPCR antibody R&D pipeline has grown rapidly with the enhancement of clinical development capabilities, and there are now more than 170 projects targeting 76 GPCR targets. But there are only 2 approved targeting-GPCR monoclonal antibodies. Another monoclonal antibody is in late stages of clinical development. Additionally, there are also multiple GPCR monoclonal antibodies in Phase 1 or 2 clinical development.
Erenumab, also called AMG-334, is a human monoclonal antibody that has been designed to bind specifically to the calcitonin gene-related peptide (CGRP) receptor (CGRPR) and antagonize the CGRP receptor. CGRP ligands are small neuropeptides with potent vasodilatory effects in chronic pain and migraine conditions. When competing with CGRP, erenumab has advantages over small-molecule drugs with specificity and potency. This antibody is indicated for the treatment of migraine, vasomotor symptoms, hot flashes and stable angina.
The monoclonal antibody was first approved in the United States and the European Union in May and July 2018, respectively; in September of the same year, the FDA approved two new migraine-targeting drugs, Teva's Ajovy (fremanezumab) and Eli Lilly&Co's Emgality (galcanezumab). Notably, Ajovy and Emgality both target CGRP, while Erenumab targets CGRPR. In addition, in 2020, the anti-CGRP monoclonal antibody drug (Eptinezumab) developed by Alder Biopharmaceuticals Inc was approved in the United States. Anti-CGRP monoclonal antibodies and CGRPR antagonists are the latest treatments for migraine.
Mogamulizumab is an anti-CC chemokine receptor 4 (CCR4) monoclonal was first approved in Japan in 2012, the trade name is Poteligeo, and it was approved by the FDA in 2018. Mogamulizumab selectively binds to and inhibits the activity of CCR4, which may block CCR4-mediated signal transduction pathways, chemokine-mediated cellular migration and proliferation of T cells, as well as chemokine-mediated angiogenesis. Additionally, this agent may induce antibody-dependent cell-mediated cytotoxicity (ADCC) against CCR4-positive T cells.
In addition to directly targeting malignant T cells expressing CCR4, mogamulizumab depletes Treg cells, an important therapeutic target in many human cancers because of their role in suppressing host anti-tumor immunity. The approved indications for this drug are CCR4-positive adult T-cell leukemia, CCR-positive peripheral T-cell lymphoma, and CCR4-positive cutaneous T-cell lymphoma. In China, the marketing application for Poteligeo (moglizumab injection) submitted by Concord Kylin (China) Pharmaceutical Co., Ltd. was accepted by the Center for Drug Evaluation (CDE) of the National Medical Products Administration (NMPA) on July 2, 2021. The monoclonal antibody is expected to become the first "first-in-class" CCR4 inhibitor in China, providing a new treatment option for patients with relapsed or refractory cutaneous T-cell lymphoma.
Leronlimab, also known as PRO140, is a humanized immunoglobulin (IgG) G4 monoclonal antibody against CC Chemokine Receptor 5 (CCR5) developed by Progenics Pharmaceuticals Inc. It acts as a human immunodeficiency virus (HIV) entry blocker and potential protective activity against graft-versus-host disease (GvHD). After administration, leronlimab targets CCR5 expressed on T cells. This blocks HIV cell entry, preventing HIV infection and/or reducing HIV viral load. Furthermore, blockade of CCR5 by leronlimab reduced CCR5-mediated signaling and CCR5-induced migration of donor cells into tissues after allogeneic hematopoietic cell transplantation (HCT). Therefore blocking CCR5 may prevent or reduce GvHD. CCR5 is a co-receptor required for HIV cell entry and plays a key role in immune regulation.
CCR5 is expressed on monocytes, activated T cells and dendritic cells (DCs) and regulates chemotaxis. Lymphocyte trafficking and recruitment to target organs through chemokine receptors (such as CCR5) play a key role in alloreactive responses. Leronlimab may also alleviate cytokine storm. Leronlimab has been developed into various clinical stages (24 clinical trials in total) for multiple diseases, including CCR5-tropic HIV infection, metastatic TNBC, metastatic colorectal cancer, nonalcoholic steatohepatitis (NASH), and graft resistance Host disease (GvHD). In 2020, leronlimab was approved for a Phase 2b/3 trial in 390 severe COVID-19 patients.
Ulocuplumab, also known as BMS-936564, is a CXCR4-specific fully human IgG4 (S224P) monoclonal antibody. CXCR4 is not only expressed on leukocytes, platelets and other non-hematopoietic cells that make up the tumor stromal microenvironment, but is also over-expressed in most human cancers. And together with its endogenous ligand CXCL12 plays a fundamental role in cancer pathogenesis involving proliferation, adhesion, metastasis, angiogenesis and survival. Ulocuplumab has been shown in patients with various hematological malignancies, including acute myeloid leukemia (AML), multiple myeloma (MM), chronic lymphocytic leukemia (CLL), follicular lymphoma (FL). Among of them, diffuse large B-cell lymphoma was evaluated in two Phase I clinical trials in subjects with primary tumor (DLBCL) and showed encouraging results. The antibody is now in Phase 2 clinical development for Waldenstrom's macroglobulinemia.
Nimacimab, also known as ryi-018, is a type 1 cannabinoid receptor (CB1) drug for kidney disease, nonalcoholic steatohepatitis, nonalcoholic steatohepatitis Liver disease, metabolic disorders, fibrosis, diabetic nephropathy and diabetic gastroparesis.
Glutazumab, also known as GMA102 or GMA105, is a novel long-acting anti-GLP-1R humanized antibody fused to a GLP-1 fragment for T2D and obesity by targeting the binding site of dual receptors to exert an antidiabetic effect. This antibody proposes an alternative targeting strategy that binds the function conferred by the antibody through fusion of a peptidyl ligand, and such a structure exhibits superior safety and tolerability over comparable GLP1 analogs.
Avdoralimab, also known as IPH-5401, is a monoclonal antibody that specifically binds to C5AR1 expressed on myeloid-derived suppressor cells (MDSCs) and neutrophils, blocking the binding of C5a to C5aR1. This drug is Initially in clinical development in Australia for rheumatoid arthritis. But now IPH-5401 is undergoing a combined phase 1/2 study (NCT03665129) and the checkpoint inhibitor durvalumab (anti-PD-L1) under the background of immuno-oncology in selected solid tumors (NSCLC, HCC, RCC, urinary epithelial cell carcinoma). Antagonism of this monoclonal antibody blocks MDSCs in the TME, thereby enhancing CD8 T cell infiltration and function.
Plozalizumab, also called MLN-1202, is a humanized monoclonal antibody that directly interacts with human chemokine receptor 2 (CCR2) and inhibits MCP-1 binding. When plozalizumab binds to CCR2 and prevents endothelial-derived CLL2 (monocyte chemoattractant protein-1 or MCP1) from binding to its receptor CCR2, it may inhibit the activation of CCR2, thereby inhibiting angiogenesis, tumor cell migration and tumor cell proliferation. This drug may also decrease C-reactive protein (CRP) levels. Although the antibody drug entered Phase II studies in multiple disease indications, two Phase II clinical trials for diabetic nephropathy (NCT02410499) and atherosclerotic cardiovascular disease (NCT02388971) have been canceled.
Volagidemab, also known as REMD-477, is a human anti-glucagon receptor antibody for juvenile type 1 diabetes (T1D) and type 2 diabetes (T2D). Its mechanism of action is to increase hepatic glucose uptake by blocking glucagon receptor (GCGR) signaling, then, reducing hepatic glycogenolysis and gluconeogenesis, and promoting glycogen synthesis to achieve hypoglycemic effect. As of March 2021, this drug has a number of experimental projects under research, among which the research and development of type 1 diabetes and type 2 diabetes is in clinical phase II, the research on glucose intolerance is in clinical phase I, and the research on metabolic disorders is In preclinical stage.
In addition, some are in clinical phase I and preclinical projects.
| Targets | Drug Names | Companies | Indications | Phases |
|---|---|---|---|---|
| CCR7 | P-007 | NB Health Laboratory Co Ltd | Kidney fibrosis; pulmonary fibrosis | Preclinical |
| CCR9 | SRB-2 | Centro Nacional de Biotecnología | T-cell acute lymphoblastic leukemia; pancreatic tumors; cancer | Preclinical |
| CXCR5 | SAR-113244 | Sanofi SA | Systemic lupus erythematosus | Phase I |
| BAY-924 | Bayer AG | B cell lymphoma | Preclinical | |
| HFB-1002 | HiFiBio | Hematological neoplasms; B-cell lymphomas; autoimmune diseases | Preclinical | |
| STI-B030X | Sorrento Therapeutics Inc | Cancer; inflammatory disease | Preclinical | |
| anti-CXCR5 chimeric antibodies (BLAST) | North Coast Biologics LLC | / | Preclinical | |
| EGFR/LGR5(Bispecific) | MCLA-158 | Merus N.V | Metastatic colorectal cancer; metastatic gastric cancer; head and neck tumors; skin lymphoma; advanced solid tumors | Phase I |
| ETaR(EDNRA) | GMA-301 | Hangzhou Gmax Biopharm Biomedical Engineering Co Ltd | Pulmonary hypertension | Phase I |
| FZD10 | OTSA-101-DTPA-90Y | University of Tokyo | Soft tissue sarcoma | Phase I |
| FZD7 | Vantictumab | OncoMed Pharmaceuticals Inc | Pancreatic neoplasms; breast neoplasms; metastatic lung cancer; solid tumors | Phase I |
| FZD8 | Ipafricept | OncoMed Pharmaceuticals Inc | Hepatocellular carcinoma; pancreatic tumor; ovarian tumor; cancer | Phase I |
| LGR5 | BNC-101 | Dyax Corp | Metastatic pancreatic cancer; colorectal neoplasms; metastatic gastrointestinal cancer; metastatic breast cancer; cancer | Phase I |
| LGR5/LGR4(Bispecific) | BNC-102 | Bionomics Ltd | Solid tumor | Preclinical |
| PTGDR2 | anti-CRTh2 antibody | Genentech | Asthma | Preclinical |
| RSPO3 | Rosmantuzumab | OncoMed Pharmaceuticals Inc | Metastatic colorectal cancer; cancer | Phase I |
As a type of important drug targets, GPCRs attract more and more attention in the field of drug development, especially in the field of monoclonal antibody drug development. Accumulating clinical drug experiments have been extended to Anti-GPCR antibody drugs. The full understanding of the biological properties of GPCRs in oncology, especially in tumor immunity, provides broad prospects for the application of therapeutic antibodies against GPCRs as monotherapy or combination therapy. The application of new-generation protein drug development strategies, such as bispecific antibodies and antibody-drug conjugates, has opened up a new field for the application of antibody drugs.


Comments
Leave a Comment