Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
Lung cancer is the leading cause of cancer deaths in both men and women in the U.S. and worldwide. It claims more lives each year than do colon, prostate, ovarian and breast cancers combined, and the cause of lung cancer is still not completely clear. For this reason, the pathogenesis and treatment of lung cancer has always been the focus of research by researchers. Here, combining with the latest research data, we discuss the lung cancer from six aspects as follows:
Lung cancer is a malignant tumor that begins in the lungs. Our lungs are two spongy organs in your chest that take in oxygen when you inhale and release carbon dioxide when you exhale. Clinically, lung cancer, also called primary bronchogenic carcinoma, is a type of cancer that originates in the bronchi and alveoli. As the figure 1 shows:
Figure 1. Lung cancer begins in the cells of your lungs
Lung cancer can occur in any lung of both lungs, but the right lung is more than the left lung, the upper lobe is more than the lower lobe, the middle lobe is the least, and the upper lobe is the most.
Clinically, lung cancer is mainly divided into non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). And non-small cell lung cancer accounts for about 85% of lung cancer.
The proliferation and expansion of NSCLC and SCLC are completely different, and the treatment measures are different.
Based on different cell morphology, NSCLC can be divided into three subtypes, including adenocarcinoma, squamous cell carcinoma and large cell carcinoma.
Adenocarcinoma, among the three subtypes, accounts for 40% of all lung cancer types, accounting for about 55% of non-small cell lung cancer. The tumors often occupy a place in the surrounding area of the lungs.
In this subtype of NSCLC, the more common mutant genes are EGFR, ALK, c-Met, ROS1, HER2, KRAS, etc., and are currently the most targeted cancer drugs. The drugs that can be used for EGFR gene mutation include gefitinib, erlotinib, and ectinib; the target drugs for ALK mutation include crizotinib, ceritinib, and erlotinib.
Squamous cell carcinoma is a common subtype of smoking. It is more common in male patients, often originates from a larger airway. Therefore it tends to occupy a central position in the lungs.
In the United States, squamous cell carcinoma accounts for about 25% to 30% of the total number of lung cancers, including papillary squamous cell carcinoma, clear cell squamous cell carcinoma, small cell squamous cell carcinoma, and basal squamous cell carcinoma.
In this subtype of NSCLC, common gene mutations include FGFR1, STK11, SOX, PIK3CA, DDR2, PDGFRA, MDM2, etc. Targeted drugs for squamous cell carcinoma are still in clinical stage.
Large cell carcinoma accounts for about 10%-15% of NSCLC, including four subtypes, clear cell large cell carcinoma, basal cell-like large cell carcinoma, pulmonary lymphoepithelial neoplasia, and lung large cell neuroendocrine carcinoma.
It appears as a highly undifferentiated or immature large cell through the microscope, and can occupy any part of the lungs without the tendency to be surrounded or centered. Currently, there is no particularly effective targeted drug for large cell lung cancer.
SCLC can observe very small cells under the microscope, and the shape of the cells is spindle-shaped or polygonal. It accounts for about 15% of the total number of lung cancers and has a high degree of malignancy and limited treatment.
Currently, there are no approved targeted drugs, and it has a good response to chemotherapy and radiotherapy. The occurrence of small cell lung cancer is closely related to smoking, and only 1% of small cell lung cancer has nothing to do with smoking.
It grows and spreads faster than non-small lung cancer, and tends to metastasize early in the disease. Most patients have already metastasized at the time of diagnosis. In addition, small cell lung cancer tends to occupy a large airway, so it is generally located in the center of the lung.
Although the pathogenesis mechanism of lung cancer is still not completely clear, we refer to the research data and pathway from KEGG and summarize several lung cancer related signaling pathways.
As mentioned before, Non-small-cell lung cancer (NSCLC) accounts for approximately 85% of lung cancer and represents a heterogeneous group of cancers, consisting mainly of squamous cell (SCC), adeno (AC) and large-cell carcinoma.
Molecular mechanisms altered in NSCLC include activation of oncogenes, such as K-RAS, EGFR and EML4-ALK, and inactivation of tumor-suppressor genes, such as p53, p16INK4a, RAR-beta, and RASSF1. Point mutations within the K-RAS gene inactivate GTPase activity and the p21-RAS protein continuously transmits growth signals to the nucleus.
Mutations or overexpression of EGFR leads to a proliferative advantage. EML4-ALK fusion leads to constitutive ALK activation, which causes cell proliferation, invasion, and inhibition of apoptosis. Inactivating mutation of p53 can lead to more rapid proliferation and reduced apoptosis.
The protein encoded by the p16INK4a inhibits formation of CDK-cyclin-D complexes by competitive binding of CDK4 and CDK6. Loss of p16INK4a expression is a common feature of NSCLC. RAR-beta is a nuclear receptor that bears vitamin-A-dependent transcriptional activity. RASSF1A is able to form heterodimers with Nore-1, an RAS effector.Therefore loss of RASSF1A might shift the balance of RAS activity towards a growth-promoting effect. As the figure 2 shows:
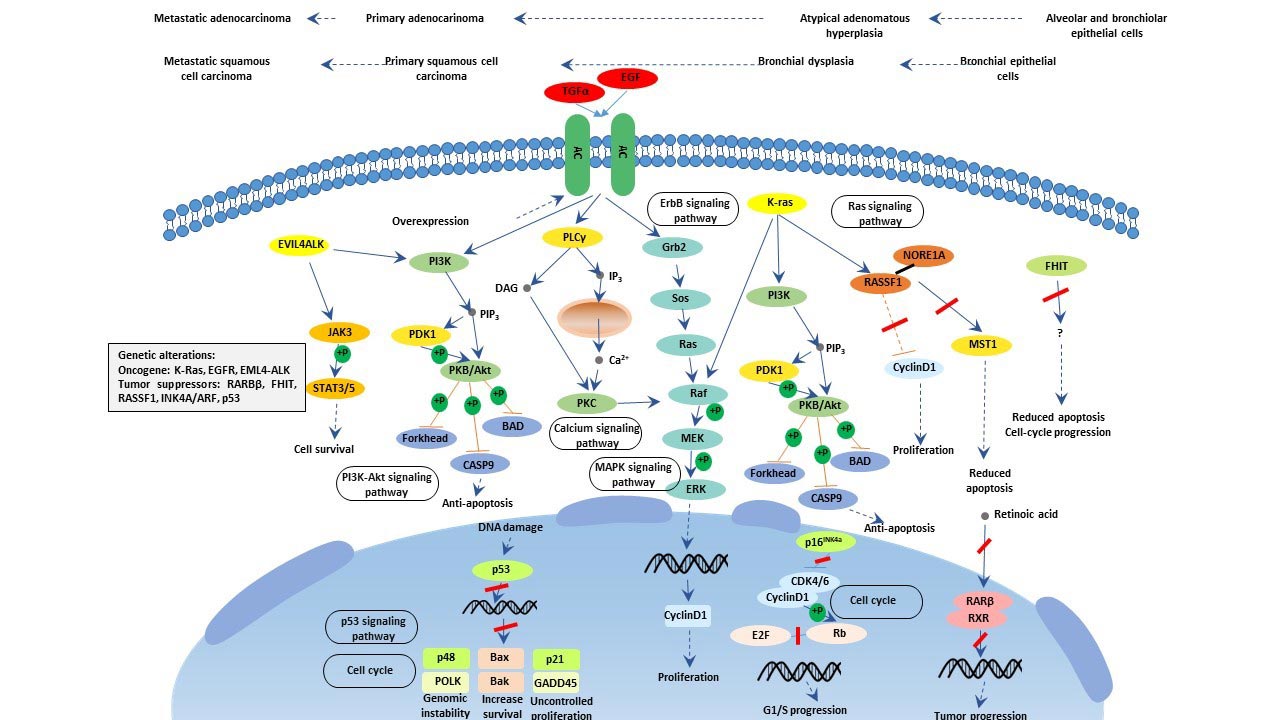
Figure 2. The diagram of NSCLC signaling pathway
PI3K-Akt signaling pathway is an intracellular signaling pathway important in regulating the cell cycle and is activated by many types of cellular stimuli or toxic insults. It regulates fundamental cellular functions, involving transcription, translation, proliferation, growth, and survival in response to extracellular signals. More information you may be interested in the article named PI3K-Akt Signaling Pathway and Cancer.
Accumulating evidence has indicated that PI3K-Akt signaling pathway is overactive in most NSCLCs, promoting proliferation, migration, invasion and resistance to therapy [1] [2] [3].
In De Marco C’s study, they found that, altogether, aberrant PI3K/AKT signaling in lung epithelial cells regulated the expression of 1,960/20,436 genes (9%), though only 30 differentially expressed genes (DEGs) (15 up-regulated, 12 down-regulated and 3 discordant) out of 20,436 that were common among BEAS-AKT1-E17K, BEAS-PIK3CA-E545K and BEAS-shPTEN cells (0.1%).
p53 is a tumor suppressor gene that is involved in the development of most cancers in humans. And it is the most frequently altered gene in human cancers. The name is due to its molecular mass. You may be interested in reading the article expounding p53 comprehensively.
The regulation mechanism and function of p53 signaling pathway are mainly characterized by cell cycle regulation, DNA damage repair, apoptosis, cell senescence, regulation of metabolism.
Recent decade years, emerging plentiful studies reveal that p53 signaling pathway plays a critical role in the pathogenesis mechanism of lung cancer. And discover several targets in lung cancer which regulate the p53 signaling pathway, such as YEATS4, TNFAIP8 and WDR79 and so on [4] [5] [6].
The MAPK signaling pathway is essential in regulating many cellular processes including inflammation, cell stress response, cell differentiation, cell division, cell proliferation, metabolism, motility and apoptosis. The role of the MAPK pathway in cancer, immune disorders and neurodegenerative diseases has been well recognized [7].
In Bhardwaj V’s study, he revealed the role of epigallocatechin-3-gallate in regulating putative novel and known microRNAs which target the MAPK pathway in non-small-cell lung cancer a549 cells by next-generation sequencing. This study identified signature microRNAs that can be used as novel biomarkers for lung cancer diagnosis [8].
The Wnt signaling pathway is a group of signal transduction pathway made of proteins that pass signals into a cell through cell surface receptors. Accumulating studies have demonstrated that abnormal activated Wnt singling pathway is closely related to the development of cardiovascular disease, liver fibrosis and cancer. You may be interested in reading the article expounding Wnt Signaling Pathway comprehensively.
A study, from McDonnell Genome Institute located in Washington University School of Medicine, has demonstrated that recurrent WNT pathway alterations are frequent in relapsed small cell lung cancer. And their results suggest WNT signaling activation as a mechanism of chemo-resistance in relapsed SCLC [9].
Lung cancer tumor markers are substances produced by cancer cells or the body's response to cancer. These markers can be detected in blood, tissues, or other bodily fluids and are often used for diagnostic, prognostic, or monitoring purposes. Here are some commonly studied lung cancer tumor markers:
CEA (Carcinoembryonic Antigen): Elevated CEA levels may indicate lung cancer, but it is not specific to lung cancer and can be found in other cancers as well.
CYFRA 21-1 (Cytokeratin Fragment 21-1): Elevated levels are associated with non-small cell lung cancer (NSCLC) and can be used for monitoring treatment response.
NSE (Neuron-Specific Enolase): Higher NSE levels may be observed in small cell lung cancer (SCLC) and certain types of NSCLC.
ProGRP (Progastrin-Releasing Peptide): Particularly useful in detecting and monitoring SCLC, ProGRP levels can indicate disease progression or response to treatment.
EGFR (Epidermal Growth Factor Receptor): Genetic mutations in EGFR are common in NSCLC, and testing for these mutations helps guide targeted therapies.
ALK (Anaplastic Lymphoma Kinase): ALK gene rearrangements occur in some NSCLC cases, and detection helps identify patients who may benefit from targeted therapies.
ROS1 (ROS Proto-Oncogene 1): ROS1 gene rearrangements are found in a subset of NSCLC, and testing is crucial for targeted therapy selection.
PD-L1 (Programmed Death-Ligand 1): PD-L1 expression is assessed to determine eligibility for immunotherapy, such as PD-1/PD-L1 inhibitors.
It's important to note that while these markers play a significant role in lung cancer diagnosis and management, they are not definitive on their own. A comprehensive approach, including imaging studies and clinical evaluation, is typically used for an accurate diagnosis and treatment plan. Additionally, ongoing research may identify new markers or refine the use of existing ones in lung cancer care.
Accumulation of Nrf2 in lung cancers stabilizes Bach1 by inducing Ho1, an enzyme that catabolizes heme. According to (Lignitto et al., 2019), Nrf2 activates a metastatic program by inhibiting heme- and Fbxo22-mediated degradation of Bach1. Ho1 inhibitors are proposed as an effective strategy to prevent lung cancer metastasis [10].
Lung cancer, responsible for about 25% of all cancer deaths, is extensively studied. (Khanmohammadi et al., 2019) conducted a review on electrochemical biosensors for detecting lung cancer biomarkers, highlighting recent advances (2010-2018) [11].
Classified into subtypes like adenocarcinoma and squamous carcinoma, lung cancer's molecular characteristics and treatment guidelines are discussed by (Ruiz-Cordero et al., 2020) [12]. Imaging tests, serum microRNAs, and LDCT screening are explored for early lung cancer detection (Asakura et al., 2020; Toumazis et al., 2020) [13-14]. The EarlyCDT-Lung test's potential in predicting lung cancer risk is assessed (Sullivan et al., 2021) [15].
(Zhao et al., 2021) systematically review the relationship between lung and gut microbiota with lung cancer[16]. In KEAP1 mutant lung cancers, the ubiquinone-FSP1 axis mediates ferroptosis and radiation resistance (Koppula et al., 2022) [17].
References
[1] De Marco C, Laudanna C, et al. Specific gene expression signatures induced by the multiple oncogenic alterations that occur within the PTEN/PI3K/AKT pathway in lung cancer [J]. PLoS One.2017, 12(6).
[2] Fan J, Bao Y, et al. Mechanism of modulation through PI3K-AKT pathway about Nepeta cataria L.'s extract in non-small cell lung cancer [J]. Oncotarget. 2017, 8(19):31395-31405.
[3] Jin X, Luan H, et al. Netrin‑1 interference potentiates epithelial‑to‑mesenchymal transition through the PI3K/AKT pathway under the hypoxic microenvironment conditions of non‑small cell lung cancer [J]. Int J Oncol.2019, 54(4):1457-1465.
[4] Pikor LA, Lockwood WW, et al. YEATS4 is a novel oncogene amplified in non-small cell lung cancer that regulates the p53 pathway [J]. Cancer Res.2013, 73(24):7301-12.
[5] Sun Y, Cao L, et al. WDR79 promotes the proliferation of non-small cell lung cancer cells via USP7-mediated regulation of the Mdm2-p53 pathway [J]. Cell Death Dis. 2017, 8(4):e2743.
[6] Xing Y, Liu Y, et al. TNFAIP8 promotes the proliferation and cisplatin chemoresistance of non-small cell lung cancer through MDM2/p53 pathway [J]. Cell Commun Signal. 2018, 16(1):43.
[7] Okimoto RA, Lin L, et al. Preclinical efficacy of a RAF inhibitor that evades paradoxical MAPK pathway activation in protein kinase BRAF-mutant lung cancer [J]. Proc Natl Acad Sci U S A. 2016, 113(47):13456-13461.
[8] Bhardwaj V, Mandal AKA. Next-Generation Sequencing Reveals the Role of Epigallocatechin-3-Gallate in Regulating Putative Novel and Known microRNAs Which Target the MAPK Pathway in Non-Small-Cell Lung Cancer A549 Cells [J]. Molecules. 2019, Jan, 24, 2.
[9] Wagner AH, Devarakonda S, et al. Recurrent WNT pathway alterations are frequent in relapsed small cell lung cancer [J]. Nat Commun. 2018, Sep 17;9(1):3787.
[10]Luca Lignitto, Sarah E LeBoeuf, Harrison Homer, et al. Nrf2 Activation Promotes Lung Cancer Metastasis By Inhibiting The Degradation of Bach1[J], CELL, 2019.
[11]Akbar Khanmohammadi, Ali Aghaie, Ensieh Vahedi, et al., Electrochemical Biosensors For The Detection Of Lung Cancer Biomarkers: A Review[J]. TALANTA, 2019.
[12]Roberto Ruiz-Cordero, Walter Patrick Devine, Targeted Therapy And Checkpoint Immunotherapy In Lung Cancer[J], SURGICAL PATHOLOGY CLINICS, 2020.
[13]Keisuke Asakura, Tsukasa Kadota, Juntaro Matsuzaki, et al. A MiRNA-based Diagnostic Model Predicts Resectable Lung Cancer in Humans with High Accuracy[J], COMMUNICATIONS BIOLOGY, 2020.
[14]Iakovos Toumazis, Mehrad Bastani, Summer S Han, Sylvia K Plevritis, Risk-Based Lung Cancer Screening: A Systematic Review[J], LUNG CANCER, 2020.
[15]Frank M Sullivan, Frances S Mair, William Anderson, et al. Earlier Diagnosis of Lung Cancer in A Randomised Trial of An Autoantibody Blood Test Followed By Imaging[J], THE EUROPEAN RESPIRATORY JOURNAL, 2021.
[16]Yue Zhao, Yuxia Liu, Shuang Li, Zhaoyun Peng,et al. Role of Lung and Gut Microbiota on Lung Cancer Pathogenesis[J], JOURNAL OF CANCER RESEARCH AND CLINICAL ONCOLOGY, 2021.
[17]Pranavi Koppula, Guang Lei, Yilei Zhang, et al. A Targetable CoQ-FSP1 Axis Drives Ferroptosis- and Radiation-resistance in KEAP1 Inactive Lung Cancers[J], NATURE COMMUNICATIONS, 2022.


Comments
Leave a Comment