

Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
September 4 annually is the World Leukemia Awareness Day. According to foreign statistics of 2021, leukemia was one of the top 10 most common cancers among men and women in the United States, and its mortality rate was also among the top 10 cancer mortality rates. Leukemia accounts for about 3% of the total incidence of tumors. The incidence of leukemia is the highest in Europe and North America, with a mortality rate of 3.2/100,000 to 7.4/100,000, and a lower incidence in Asia and South America, with a mortality rate of 2.8/100,000 to 4.5/100,000.
Herein mainly introduce the definition, classification, identification, progression process, current mainstream treatment of leukemia.
The term leukemia originates from the Greek words for "white" (leukos) and "blood" (haima). Leukemias are a group of blood cancers characterized by abnormal proliferation and differentiation of hematopoietic cells due to several factors, including chromosomal abnormalities and transcription factor alterations, which lead to anemia, neutropenia, and thrombocytopenia. It begins in the bone marrow and usually affects immature white blood cells.
Different from other cancers like lung, liver, and breast cancer, which form solid tumors when they metastasize to distant organs in the body, leukemia spread throughout the body along the bloodstream and only rarely develops into solid tumors.
Leukemia symptoms are often vague and not specific. You may overlook early leukemia symptoms because they may resemble symptoms of the flu and other common illnesses. Sometimes leukemia is discovered during blood tests for some other condition.
Leukemia symptoms vary, depending on the type of leukemia. Common leukemia signs and symptoms include fever or chills, persistent fatigue, weakness, recurrent infections, unintended weight loss, swollen lymph nodes, enlarged liver or spleen, easy bleeding or bruising, recurrent nosebleeds, petechiae in the skin, excessive sweating (especially at night), bone pain, or tenderness.
Leukemia belongs to a blood disease and won't infect directly. It only inherits the susceptibility of leukemia rather than leukemia itself. Although leukemia is still a worldwide difficult miscellaneous disease and it is very difficult to treat, it is not an incurable disease.
The exact cause of leukemia is unknown. Apart from the hereditary component, there are also multiple risk factors for this disease, including gender, age, genetic disorders, medical history, and chemical exposure.
Clinically and pathologically, the classification of leukemia cases is based on the progression speed of the disease (acute or chronic) and the type of blood stem cell that they come from (myeloid cells or lymphoid cells). Each type of leukemia type shows differences in pathogenesis, origin, incidence, and prognosis.
Leukemia is broadly divided into four main subtypes:
Acute myeloid leukemia (AML)
AML is characterized by the clonal expansion of myeloblasts in the bone marrow. It is the most common form of acute leukemia in older adults (over 75) and causes the largest number of deaths from leukemia each year in the United States.
Acute lymphocytic leukemia (ALL)
ALL is the most common type of leukemia in children, teens, and young adults and in developing countries, with the highest frequency between the ages of 2 and 5 [1]. About 60% of cases are in children. It usually advances quickly and needs rapid treatment.
Chronic myeloid leukemia (CML)
CML is extremely rare, with only several thousand diagnoses each year. It affects mostly older adults and is rarely diagnosed among children and young adults. It accounts for approximately 15% of all leukemias in the U.S. All CML patients will have the "Philadelphia-positive", which is characterized by the translocation of chromosomes 9 and 22.
Chronic lymphocytic leukemia (CLL)
CLL is the most frequent leukemia in adults in Western countries. It is mostly diagnosed in people over 70 years of age and is more seen in males than in females. Approximately 10% of people who develop CLL have a family history of the disease [2]. Some cases remain stable for years and will not need treatment.
Different leukemia types vary in the progression of the disease, the treatment methods, and the harm to the patients. Therefore, it is necessary to distinguish the type of leukemia to get better symptomatic treatment. So, how to identify the type of leukemia?
Leukemia diagnosis includes blood tests (e.g. complete blood count (CBC) and blood smear), bone marrow biopsy, spinal tap, and imaging tests (CT, MRI, and PET scans).
A doctor should consider leukemia if a patient has specific clinical signs, including pale skin, enlarged lymph nodes, swollen gums, an enlarged liver or spleen, bleeding, apparent bruises, fever, ongoing infections, fatigue, or a small pinpoint rash. The patient will be suggested to have hematologic tests.
An abnormal white cell count on a blood test may point to the diagnosis. Chest CT and abdominal B ultrasound examinations can assist to observe whether there is leukemia infiltration-caused liver and spleen lymphadenopathy.
A needle biopsy and aspiration of bone marrow from a pelvic bone will be required to confirm the diagnosis and determine the precise kind of leukemia. The bone marrow examination will be carried out for leukemic cells, DNA markers, and chromosome abnormalities. Immunophenotyping/cytochemistry also be used for auxiliary diagnosis.
Normally, the blood stem cells in the bone marrow develop into red blood cells that deliver oxygen throughout the body, white blood cells that fight infections, and platelets that assist in blood clotting.
Leukemia occurs when the blood stem cells can not properly form functioning red blood cells, white blood cells, and platelets.
Like other cancers, leukemogenesis is a complex process that involves many factors and genes. According to existing research, the occurrence of leukemia is related to ionizing radiation, chemical exposure, viral infection, environmental factors, and genetic factors.
Damage or mutation occurring to the DNA of developing blood cells leads to the generation of immature blood cells, also known as blasts or leukemia cells, which grow and divide uncontrollably. Rapid and unrestrained proliferation, differentiation disorder, and inhibition of apoptosis of leukemia cells make them accumulate in the bone marrow, suppressing normal hematopoietic functions and crowding out the healthy blood cells, eventually outnumbering the healthy blood cells and leading to the symptoms of leukemia.
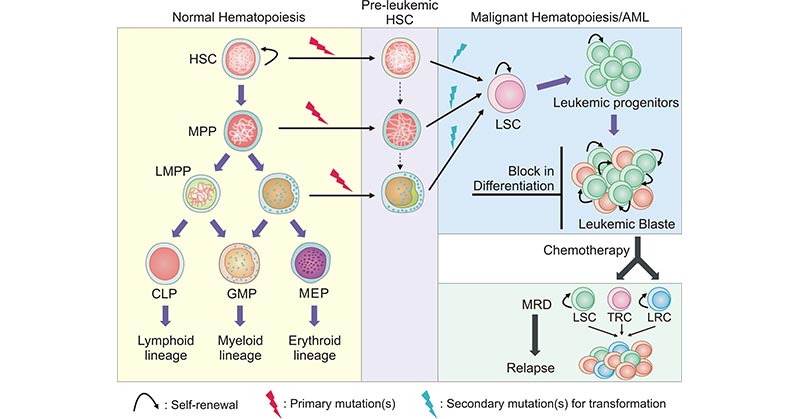
(Annotation: HSC, hematopoietic stem cell; MPP, hematopoiesis multipotent progenitor; LMPP, lymphoid-primed multipotent progenito; CMP, common myeloid progenitor; CLP, common lymphoid progenitors; GMP, granulocyte-monocyte progenitor; MEP, megakaryocyte-erythrocyte progenitor; LSC, leukemia stem cell; MRD, minimal residual disease; TRC, therapy resistant cell; LRC, leukemic-regenerating cell)
Figure 1. Process of normal hematopoiesis and leukemogenesis
This picture is cited from: https://link.springer.com/article/10.1007/s12015-021-10308-6
This leads to a deficiency of these mature blood cells, a condition known as pancytopenia. A low level of circulating red blood cells is called anemia. Leukopenia indicates a low level of white blood cells. A low level of platelets is called thrombocytopenia.
In addition to proliferation and accumulation in the bone marrow, leukemia cells can also infiltrate other non-hematopoietic tissues and organs to further inhibit the normal hematopoietic function, causing anemia, bleeding, infection, fever, liver and spleen enlargement, lymphadenopathy, systemic bone pain, and other leukemia symptoms.
Some genes are related to the prognosis of leukemia, and some can be used as molecular biological markers for leukemia to detect the existence of minimal residual disease (MRD). For example, FLT3, NPM1, CEBPA, RUNX1, ASXL1, and TP53 genes have been detected mutated in AML [3]. These gene alterations contribute to the proliferation and spread of AML in the body. CD33, CD38, CD123, and TIM3 have been identified as membrane makers for leukemia stem cells in AML [4-6].
In 2018, Mi Deng et al. identified a novel target for the treatment of acute myeloid leukemia - LILRB4 and showed that LILRB4 orchestrates tumor invasion pathways in monocytic leukemia cells by creating an immune-suppressive microenvironment [7].
It is complex to treat leukemia. Treatment for leukemia is dependent on the type of leukemia and other factors, including age and overall health of the patients, as well as whether leukemia has spread to other organs or tissues.
Therapies for leukemia include chemotherapy, radiation, biological therapy, targeted therapy, stem-cell transplant, or a combination of therapies.
Chemotherapy has a quick curative effect and great side effects. Bone marrow transplants are expensive and dangerous. The curative effect of traditional Chinese medicine is relatively slow, but it can be adjusted comprehensively, with few side effects, little pain, and low cost. A large number of medical practice has demonstrated that the method of integrated traditional Chinese and western medicine is more ideal and effective, and has small side effects.
Bone marrow transplantation is considered to be the best treatment for leukemia, but this treatment has major limitations, including the patient's condition, matching donor bone marrow, rejection after transplantation, and expensive treatment costs. The success rate of bone marrow transplantation in leukemia patients is about 60 to 70%, which is significantly related to the age of the patient, the disease status before transplantation, the extent to which the patient's bone marrow matches the donor's bone marrow, and the complications after transplantation.
At present people tend to use retinoic acid RA and arsenic agents to process targeted treatment for this disease. The patients who accept this kind of treatment can recuperate health.
On February 17, 2022, Immuno-Onc's IO-202 received fast-track designation from the FDA for the treatment of patients with relapsed or refractory acute myeloid leukemia.
IO-202 is a novel bone marrow checkpoint inhibitor targeting LILRB4. In the treatment of hematological tumors, this drug can convert the inhibitory signals received by T cells from cancer cells into activation signals, activate the killing function of T cells, and inhibit the infiltration of blood cancer cells.
CUSABIO provides a series of products for the leukemia-associated research, including ELISA kits, recombinant proteins, and antibodies.
References
[1] Inaba H, Greaves M, Mullighan CG. Acute lymphoblastic leukaemia [J]. Lancet. 2013;381(9881):1943–55.
[2] Cerhan JR, Slager SL. Familial predisposition and genetic risk factors for lymphoma [J]. Blood. 2015;126(20):2265–73.
[3] Yu, J., Li, Y., Zhang, D. et al. Clinical implications of recurrent gene mutations in acute myeloid leukemia [J]. Exp Hematol Oncol 9, 4 (2020).
[4] Liu, Y., Wang, G., Zhang, J. et al. CD9, a potential leukemia stem cell marker, regulates drug resistance and leukemia development in acute myeloid leukemia [J]. Stem Cell Res Ther 12, 86 (2021).
[5] Yahui Ding, Huier Gao, and Quan Zhang. The biomarkers of leukemia stem cells in acute myeloid leukemia [J]. Stem Cell Investig. 2017; 4: 19.
[6] Kikushige Y, Shima T, et et al. TIM-3 is a promising target to selectively kill acute myeloid leukemia stem cells [J]. Cell Stem Cell. 2010;7:708–17.
[7] Mi Deng, Xun Gui, et al. LILRB4 signaling in leukemia cells mediates T cell suppression and tumor infiltration [J]. Nature. 2018 Oct; 562(7728): 605–609.
Comments
Leave a Comment