Dengue virus (DENV) is a mosquito-borne, single positive-stranded RNA virus of the family Flaviviridae.[1] Dengue virus has increased dramatically within the last 20 years, becoming one of the worst mosquito-borne human pathogens with which tropical countries have to deal. Dengue is often a leading cause of illness in areas with risk. Forty percent of the world's population, about 3 billion people, live in areas with a risk of dengue. Each year, up to 400 million people get infected with dengue. Approximately 100 million people get sick from infection, and 22,000 die from severe dengue.
1. The Structure and Important Proteins
The DENV genome is about 11000 bases of positive-sense, single stranded RNA that codes for three structural proteins (capsid protein C, membrane protein M, envelope protein E) and seven nonstructural proteins (NS1, NS2a, NS2b, NS3, NS4a, NS4b, NS5) [2]. It also includes short noncoding regions on both the 5' and 3' ends [1].

Figure 1. The Structure Comparison of DENV
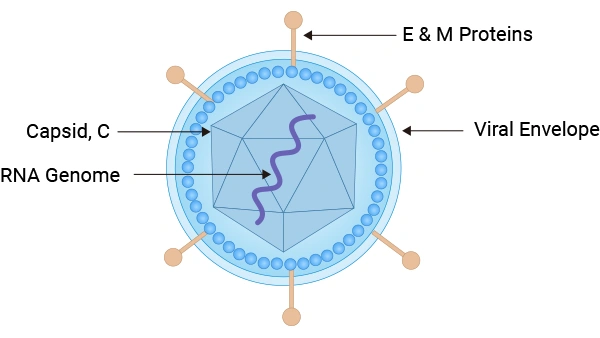
Figure 2. Dengue Virus Structure
2. Mechanisms of Dengue Virus
Dengue virus pathogenesis involves complex interactions between the virus and host cellular and immune responses. The viral life cycle consists of several key stages:
1
Entry
The virus enters host cells through receptor-mediated endocytosis involving attachment factors such as DC-SIGN.
2
Uncoating and Translation
In the acidic endosome, the virus uncoats, In the acidic endosome, viral uncoating releases the RNA genome, which is translated into a single polyprotein and subsequently cleaved into structural and non-structural proteins at the endoplasmic reticulum.
3
Replication and Packaging
NS5 (polymerase) and NS3 (helicase) cooperate to amplify the viral RNA, while the capsid protein (C) facilitates nucleocapsid assembly on the surface of lipid droplets.
4
Maturation and Release
Immature virions undergo maturation in the Golgi apparatus through prM cleavage, and are ultimately released via exocytosis.
These processes are critical for viral propagation and provide multiple targets for antiviral intervention, including NS5 polymerase and host lipid metabolism pathways such as FADS2.
3. Related Products
● Dengue Virus Recombinant Proteins
● Dengue Virus Antibodies
4. Dengue virus in Disease Research
Dengue fever is a mosquito-borne tropical disease caused by the dengue virus. People of all ages who are exposed to infected mosquitoes are possible victims of dengue fever. Typically, people infected with dengue virus are asymptomatic or have only mild symptoms such as an uncomplicated fever [3]. Others have more severe illness (5%), and in a small proportion it is life-threatening.
Symptoms typically begin 3 to 14 days after infection. These may include a high fever, headache, vomiting, muscle and joint pains, and a characteristic skin rash.
In a small proportion of cases, the disease develops into severe dengue, also known as dengue hemorrhagic fever, resulting in bleeding, low levels of blood platelets and blood plasma leakage, or into dengue shock syndrome, where dangerously low blood pressure occurs.
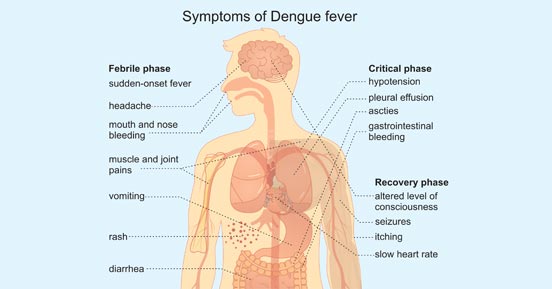
Figure 3. Symptoms of Dengue Fever
5. Dengue virus Transmission
Through Mosquito Bites
Dengue viruses are spread to people through the bites of infected Aedes mosquitos, particularly A. aegypti. Other Aedes species that transmit the disease include A. albopictus, A. polynesiensis and A. scutellaris. Mosquitoes become infected when they bite a person infected with the virus. Infected mosquitoes can then spread the virus to other people through bites.
From mother to child
A pregnant woman already infected with dengue can pass the virus to her fetus during pregnancy or around the time of birth. And dengue spread through breast milk has been reproted [4]. When a mother does have a DENV infection when she is pregnant, babies may suffer from pre-term birth, low birthweight, and fetal distress.
Through infected blood
Dengue can also be transmitted via infected blood products and through organ donation [5]. In countries such as Singapore, where dengue is endemic, the risk is estimated to be between 1.6 and 6 per 10,000 transfusions [6].
Others
Other person-to-person modes of transmission, including sexual transmission, have also been reported, but are very unusual [7].
FAQ: Ebola virus
Q:How many serotypes of the dengue virus are there, and what are their research implications?
The dengue virus (DENV) is classified into four serotypes: DENV-1, DENV-2, DENV-3, and DENV-4, all of which are single-stranded positive-sense RNA viruses. While the four serotypes cause similar clinical symptoms, they differ antigenically. Secondary infection with a heterologous serotype significantly increases the risk of severe dengue. In research, each serotype is often studied individually for vaccine development, diagnostic assay development, and antibody characterization.
Q:What are the key proteins of the dengue virus, and which are commonly targeted in research?
The structural proteins include C protein, M protein, and E protein. The non-structural proteins include NS1, NS2A/B, NS3, NS4A/B, and NS5. Common research targets are:
E protein – involved in receptor binding and a target for neutralizing antibodies.
NS1 – used for antigen detection, and involved in pathogenesis and immune evasion.
NS3/NS5 – replication enzymes and drug targets.
C protein – involved in viral assembly.
Q:What detection methods are commonly used in dengue virus research, and how do their applicable stages differ?
Common methods include:
Nucleic acid PCR – high sensitivity, suitable for early-stage infection.
Antigen detection (e.g., NS1) – typically detectable during the first 1–7 days after symptom onset.
Antibody detection (IgM/IgG) – generally useful from 5–7 days after infection for clinical diagnosis and seroepidemiological studies.
Virus isolation – the gold standard, but time-consuming.
Q:Why are NS3 and NS5 of the dengue virus frequently targeted for drug development?
NS3 possesses protease, NTPase, and helicase activities, responsible for viral polyprotein cleavage and RNA unwinding. NS5 functions as an RNA-dependent RNA polymerase, driving viral RNA replication and suppressing host antiviral responses. Both proteins are essential for viral replication and are key targets for small-molecule antiviral development.
References:
[1] Rodenhuis-Zybert IA, Wilschut J, Smit JM. Dengue Virus Life Cycle: Viral and Host Factors Modulating Infectivity [J]. Cell Mol Life Sci, 67 (16), 2773-86.
[2] Dwivedi, VD, Tripathi, IP, Tripathi, RC, et al. Genomics, proteomics and evolution of dengue virus. Briefings in Functional Genomics, July 2017, Pages 217–227.
[3] Senanayake A M Kularatne. Dengue Fever. BMJ, 351, h4661.
[4] Viroj Wiwanitkit. Unusual Mode of Transmission of Dengue. J Infect Dev Ctries, 4 (1), 51-4.
[5] Annelies Wilder-Smith, Lin H Chen, Eduardo Massad, et al. Threat of Dengue to Blood Safety in Dengue-Endemic Countries [J]. Emerg Infect Dis, 15 (1), 8-11.
[6] D Teo, L C Ng, S Lam. Is Dengue a Threat to the Blood Supply [J]. Transfus Med, 19 (2), 66-77.
[7] Lin H Chen, Mary E Wilson. Dengue and Chikungunya Infections in Travelers [J]. Curr Opin Infect Dis, 23 (5), 438-44.
