Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
Severe acute respiratory syndrome-related coronavirus (SARSr-CoV) is a species of coronavirus, it is a member of the genus Betacoronavirus and subgenus Sarbecoronavirus. SARSr-CoV is an enveloped positive-sense single-stranded RNA virus that enters its host cell by binding to the ACE2 receptor, then infects humans, bats and certain other mammals. [1] Bats are a major reservoir of many strains of SARS-related coronaviruses. Only recently have strains of SARS-related coronavirus evolved and made the cross-species jump from bats to humans, as in the case of the strains SARS-CoV and SARS-CoV-2. [2]
SARS-CoV and SARS-CoV-2 have caused outbreaks of severe respiratory diseases in humans: SARS-CoV (or SARS-CoV-1), which caused an outbreak of severe acute respiratory syndrome (SARS) between 2002 and 2003, and SARS-CoV-2, which caused the 2019–20 pandemic of coronavirus disease 2019 (COVID-19).
In this article, we mainly discuss SARS-CoV, including structure, the important proteins, infection mechanisms, infection Symptoms, transmission, Diagnosis and Treatment. If you want to know more about SARS-CoV-2, please click 2019 Novel Coronavirus.
The SARS-related coronavirus is an enveloped, positive-sense, single-stranded RNA virus. Its genome is about 30 kb, which is one of the largest among RNA viruses.
The viral envelope consists of a lipid bilayer where the membrane (M), envelope (E) and spike (S) proteins are anchored. [3] The spike protein's interaction with its complement host cell receptor is central in determining the tissue tropism, infectivity, and species range of the virus. [4] Inside the envelope, there is the nucleocapsid, which is formed from multiple copies of the nucleocapsid (N) protein. The lipid bilayer envelope, membrane proteins, and nucleocapsid protect the virus when it is outside the host. [5]
Follows the replication strategy typical of the coronavirus subfamily, the primary human receptor of SRAS-CoV is angiotensin-converting enzyme 2 (ACE2), first identified in 2003. [6]
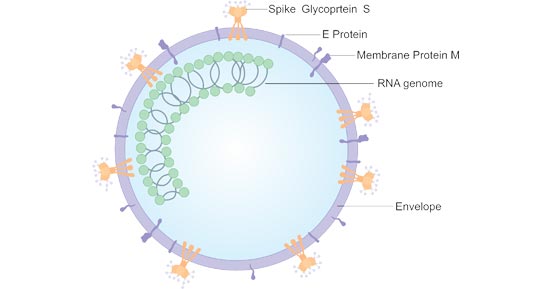
Figure 1. The Structure of SARS-CoV
| Target | Uniprot No. | Protein Name | Description |
|---|---|---|---|
| 1a | P0C6U8 | Replicase polyprotein 1a | The papain-like proteinase (PL-PRO) is responsible for the cleavages located at the N-terminus of replicase polyprotein. |
| 3a | P59632 | Protein 3a | Forms homotetrameric potassium sensitive ion channels and may modulate virus release. Up-regulates expression of fibrinogen subunits FGA, FGB and FGG in host lung epithelial cells. |
| 3b | P59633 | Non-structural protein 3b | Induces host cell G0/G1 arrest and apoptosis |
| 6 | P59634 | Non-structural protein 6 | Could be a determinant of virus virulence. |
| 7a | P59635 | Protein 7a | Non-structural protein which is dispensable for virus replication in cell culture. |
| 7b | Q7TFA1 | Protein non-structural 7b (E.coli) | |
| 8a | Q7TFA0 | Protein non-structural 8a | |
| 8b | Q80H93 | Non-structural protein 8b | |
| 9b | P59636 | Protein 9b | The gene encoding this protein is included within the N gene. |
| E | P59637 | Envelope small membrane protein | Plays a central role in virus morphogenesis and assembly. |
| M | P59596 | Membrane protein | Component of the viral envelope that plays a central role in virus morphogenesis and assembly via its interactions with other viral proteins. |
| N | P59595 | Nucleoprotein (N) (Baculovirus) | Packages the positive strand viral genome RNA into a helical ribonucleocapsid and plays a fundamental role during virion assembly through its interactions with the viral genome and membrane protein M. |
| ORF14 | Q7TLC7 | Uncharacterized protein 14 | / |
| rep | P0C6X7 | Replicase polyprotein 1ab | Multifunctional protein involved in the transcription and replication of viral RNAs. Contains the proteinases responsible for the cleavages of the polyprotein. |
| S | P59594 | Attaches the virion to the cell membrane by interacting with host receptor, initiating the infection. | |
| N/A | C8YZ74 | 3C-like proteinase (in vitro E.coli expression system) | / |
Severe acute respiratory syndrome (ARS) is the disease caused by SARS-CoV. The illness usually begins with a high fever, sometimes associated with chills or other symptoms, including headache, general feeling of discomfort, and body aches. Some people also experience mild respiratory symptoms at the outset. Diarrhea is seen in approximately 10% - 20% of patients. After 2 to 7 days, SARS patients may develop a dry, nonproductive cough that might be accompanied by or progress to a condition in which the oxygen levels in the blood are low . In 10% - 20% of cases, patients require mechanical ventilation. Most patients develop pneumonia.
In the SARS outbreak of 2003, about 9% of patients with confirmed SARS-CoV infection died. [7] The mortality rate was much higher for those over 60 years old, with mortality rates approaching 50% for this subset of patients.In the SARS outbreak of 2003, about 9% of patients with confirmed SARS-CoV infection died.[7] The mortality rate was much higher for those over 60 years old, with mortality rates approaching 50% for this subset of patients.
Transmission of SARS-CoV is primarily from person to person.
SARS-CoV is thought to be transmitted most readily by respiratory droplets produced when an infected person coughs or sneezes. Droplet spread can happen when droplets from the cough or sneeze of an infected person are propelled a short distance through the air and deposited on the mucous membranes of the mouth, nose, or eyes of persons who are nearby.
The virus also can spread when a person touches a surface or object contaminated with infectious droplets and then touches his or her mouth, nose, or eyes.
In addition, it is possible that SARS-CoV might be spread more broadly through the air or by other ways that are not now known.
References
[1] Wong AC, Li X, Lau SK, et al. Global Epidemiology of Bat Coronaviruses [J]. Viruses. 2019 Feb; 11(2): 174.
[2] Cui J, Han N, Streicker D, Li G, et al. Evolutionary Relationships between Bat Coronaviruses and Their Hosts [J]. Emerg Infect Dis. 2007 Oct; 13(10): 1526–1532.
[3] Lai MM, Cavanagh D. The molecular biology of coronaviruses [J]. Adv Virus Res. 1997;48: 1-100.
[4] Jie Cui, Fang Li, Zheng-Li Shi. Origin and evolution of pathogenic coronaviruses [J]. Nat Rev Microbiol. 2019; 17(3): 181–192.
[5] Neuman BW, Kiss G, Kunding AH, et al. A structural analysis of M protein in coronavirus assembly and morphology [J]. J Struct Biol. 2011 Apr; 174(1): 11–22.
[6] Li, Wenhui, Moore, Michael J, et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus [J]. Nature. 2003; 426(6965): 450–454.
[7] Sørensen MD, Sørensen B, Gonzalez-Dosal R, et al. Severe acute respiratory syndrome (SARS): development of diagnostics and antivirals [J]. Ann N Y Acad Sci. 2006 May;1067: 500-5.
Proteins
Antibodies
ELISA Kits