

Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)
Coronary heart disease (CHD) is a leading cause of death worldwide. Among the CHD, myocardial infarction (MI) is the most common form. Data from the United States indicates that about 25% of deaths in the United States are related to heart disease annually [1]. Within the heart disease spectrum, an American has a myocardial infarction every 40 seconds, according to the 2020 heart disease and stroke statistics from the American Heart Association (AHA) [2].
A myocardial infarction, medically known as heart attack, refers to myocardium necrosis due to prolonged ischemia resulting from coronary artery occlusion. In most cases, myocardial infarction suddenly occurs, also called an acute myocardial infarction (AMI). A myocardial infarction might lead to permanent cardiac damage and perhaps death if blood flow isn't rapidly restored. Early diagnosis and timely treatment of a myocardial infarction are essential and can save a person's life. Without treatment, a myocardial infarction can result in cardiac arrest, in which the heart stops beating entirely.
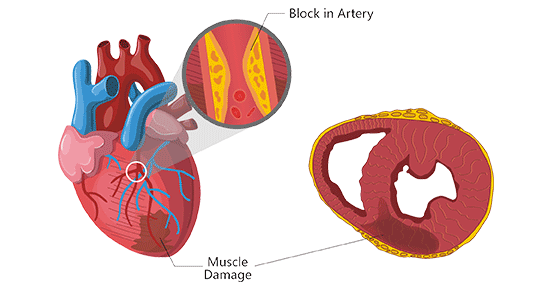
Figure: Myocardial infarction
This picture is cited from: https://en.wikipedia.org/wiki/Myocardial_infarction
There are two types of myocardial infarction: ST-segment elevated myocardial infarction (STEMI) and non-ST segment elevated myocardial infarction (NSTEMI). "ST segment" is part of the electrocardiograph (ECG) heart tracing used to diagnose a heart attack.
STEMI
A STEMI occurs when atherosclerotic plaque erosion, cracks, ulcers, or dissections cause acute occlusive thrombosis in one or more coronary arteries, thereby interrupting blood supply. STEMI patients usually manifest persistent chest discomfort, palpitations, chest pain, arrhythmia, and hypotension. It is a fatal cardiovascular emergency. Once it occurs, early diagnosis and rapid reperfusion therapy are required. The STEMI treatments aim to restore myocardial blood perfusion as soon as possible to save dying myocardium, blocking infarction from expanding, protecting and maintaining cardiac function, dealing with severe arrhythmia, heart failure, and various complications in time, thereby preventing sudden death.
NSTEMI
An NSTEMI is caused by severe coronary artery narrowing, transient occlusion, or microembolization of thrombus and atheromatous material. It can cause the symptoms of a classic heart attack but tends to inflict less damage to myocardia. NSTEMI is defined by an increase of cardiac biomarkers in the absence of ST elevation. The NSTEMI treatments aim to immediately relieve ischemia and prevent myocardial infarction or reinfarction. Treatment of NSTEMI includes antiischemic therapy, antithrombotic therapy, and risk stratification-based invasive therapy.
So far, atherosclerosis is the most common cause of myocardial infarction. Endothelial dysfunction and inflammation lead to lipid accumulation in the vessel walls resulting in the formation of an atherosclerotic plaque made up of a central lipid core surrounded by foamy macrophages and smooth muscle cells covered by a fibrous cap [3]. Plaque shedding and rupture trigger platelet adhesion and aggregation and activation of the coagulation system, which induces thrombosis and leads to coronary lumen stenosis or occlusion [4]. This is often attributed to longstanding coronary artery disease (CAD). Narrowing of coronary arteries and occlusion of blood flow causes persistent myocardial ischemia and hypoxia. An inadequate supply of oxygen for a given myocardial demand results in myocardial ischemia and myocardium necrosis, eventually causing myocardial infarction.
Electrocardiogram (ECG) is the gold standard for the diagnosis of myocardial infarctionI within 6 hours after myocardial infarction. Myocardial injury markers provide the basis for the diagnosis of myocardial infarction. Clinical symptoms, ECG changes, and elevation of myocardial injury markers can be combined to diagnose myocardial infarction.
After myocardial cell injury, various components of the cells enter the blood circulation, some of which can reflect myocardial injury more specifically and sensitively and are called myocardial injury markers. The application of myocardial injury markers has experienced from aspartate transferase (AST) to lactate dehydrogenase (LD), to myoglobin (Mb), creatine kinase (CK), myocardial creatine kinase isoenzyme (CK-MB), and myocardial creatine kinase isoenzyme mass (CK-MB mass), and finally to the development process of cardiac troponin (cTn). In addition, heart-type fatty acid-binding protein (H-FABP) acts as a diagnostic indicator of early AMI is used in clinical practice, and high-sensitivity C-reactive protein (hs-CRP) is mainly used to diagnose and predict the occurrence and progression of cardiovascular events.
The serological examination is particularly important for those patients with atypical clinical manifestations and ECG. The rational use of myocardial injury markers can effectively reduce the mortality of patients with myocardial infarction. The following table shows the elevation of different markers of myocardial injury at different periods after myocardial infarction.
| Myocardial Injury Markers | Elevated Period | Peak Period | Duration of elevation | Specificity | Sensitivity | Clinical Significance |
|---|---|---|---|---|---|---|
| AST/GOT | 6-12h | 24-48h | 5-7d | Low (+) | Low (++) | Not tissue-specific, a simple increase in AST cannot diagnose myocardial injury |
| CK | 3-8h | 10-36h | 3-4d | Low (++) | Low (++) | If the concentration of CK at 24 hours after AMI is less than the upper limit of the reference value, AMI can be excluded. |
| CK-MB | 3-8h | 9-30h | 2-3d | High (++++) | Relatively high (+++) |
|
| LDH | 6-10h | 2-3d | 7-14d | Low (+) | Low (++) |
|
| LDH1 | 8-12h | 2-3d | 7-12d | Low | Low | Serum LD1 and LD2 increase during the AMI early stage, but LD1 increases earlier and more significantly, leading to the increase of LD1/LD2 ratio. Therefore, LD1/LD2 ≥ 1 is a specific indicator for the diagnosis of myocardial infarction. |
| Mb | 0.5-2h | 6-12h | 1d | Low (+) | Relatively high (+++) |
|
| cTn-I | 3-8h | 12-24h | 7-10d | High (+++++) | High (++++) |
|
| cTn-T | 3-8h | 24-48h | 10-14d | Relative high (+++) | High (++++) |
|
| NT-proBNP |
NT-proBNP < 300pg/ml, exclude the possibility of acute heart failure, a high negative predictive value, Patient age < 50 years old, NT-proBNP ≥450pg/ml, indicating heart failure Patients age: 50 to 75 years, NT-proBNP ≥900pg/ml, indicating severe heart failure Patient age >75 years old, NT-proBNP ≥1800pg/ml, high risk of AMI |
|
||||
| CRP | 4-6h | 3-4d | 7-10d | Low (++) | Relatively high (+++) |
|
| H-FABP | 1-3h | 6-8h | 24-30h | Low (++) | Relatively high (+++) |
|
An ideal myocardial injury marker is characterized by high myocardial specificity and sensitivity, available to detect early myocardial injury, a long window period, ability to rapidly clear from the blood and be indicators for the diagnosis of recurrence. Because a single marker cannot meet all the above conditions, multiple myocardial injury markers are generally combined to assist clinical diagnosis. Combined detection of CK-MB, Mb, cTnI and BNP/ NT-proBNP levels can significantly promote the early diagnosis of AMI and provide clinical diagnostic evidence, thus reducing the mortality of AMI.
CUSABIO provides a batch of ELISA kits designed to detect markers of myocardial infarction for scientific research purposes.
Further reading:
References
[1] Benjamin EJ, Blaha MJ, et al. Heart disease and stroke statistics-2017 update: A report from the American Heart Association [J]. Circulation. 2017 Mar 7; 135(10): e146–e603.
[2] Virani SS, et al. Heart disease and stroke statistics‐2020 update: a report from the American Heart Association [J]. Circulation. 2020;141(9):e139‐e596.
[3] Lina Badimon, Teresa Padró, and Gemma Vilahur. Atherosclerosis, platelets and thrombosis in acute ischaemic heart disease [J]. Eur Heart J Acute Cardiovasc Care. 2012 Apr; 1(1): 60–74.
[4] Goldstein JA, Demetriou D, et al. Multiple complex coronary plaques in patients with acute myocardial infarction [J]. New England Journal of Medicine 2000; 343:915-922.
[5] Okamoto F, Sohmiya K, Ohkaru Y, et al. Human heart-type cytoplasmic fatty acid-binding protein (H-FABP) for the diagnosis of acute myocardial infarction. Clinical evaluation of H-FABP in comparison with myoglobin and creatine kinase isoenzyme MB[J]. Clinical Chemistry & Laboratory Medicine Cclm, 2000, 38(3):231-8.
Comments
Leave a Comment