Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)

Crimean-Congo hemorrhagic fever (CCHF) is a tick-borne disease caused by the Crimean-Congo hemorrhagic fever virus (CCHFV). It has an exceptionally broad geographic distribution, spanning more than 30 countries across Asia, Europe, the Middle East, and Africa. Emerging cases continue to appear in traditionally non-endemic regions, making CCHF an increasingly pressing global public health challenge. The disease is notable for its high case fatality rate and widespread potential threat, and has been classified by the World Health Organization as a priority pathogen [1]. Currently, no approved specific antiviral drugs or vaccines are available worldwide.
CCHFV is a segmented negative-sense RNA virus with a genome consisting of three segments:
S segment: Encodes the nucleocapsid protein (NP), which is highly conserved and serves as a core target for serological detection.
M segment: Encodes the glycoprotein precursor (GPC), which undergoes proteolytic processing to produce Gn and Gc, involved in receptor binding and membrane fusion.
L segment: Encodes the RNA-dependent RNA polymerase (RdRp).
The virus is primarily transmitted through the bite of Hyalomma ticks, but can also spread through human-to-human transmission via contact with infected animal blood or bodily fluids from patients. The host range is broad, including cattle, goats, sheep, wild boar, rabbits, and dromedary camels.
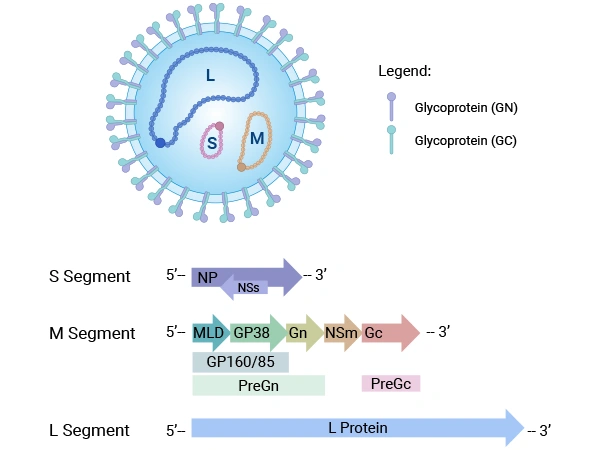
Figure caption: Virion structure of Crimean-Congo hemorrhagic fever virus (CCHFV) [2].
Source: PMID:37753088
CCHF is a zoonotic disease whose distribution is closely linked to that of its tick vectors. CCHFV is found in over 30 countries across Africa, Asia, Southern Europe, and the Middle East, and is primarily transmitted by ticks of the Hyalomma genus [3]. Climate change and livestock trade may accelerate its spread into new regions. The virus can be maintained in an enzootic cycle involving ticks, mammals, and birds.
Human infection can occur through the following routes: tick bites, contact with the blood or bodily fluids of infected patients or animals, and nosocomial (hospital-acquired) transmission.
Of note, the virus exhibits considerable stability on inanimate surfaces. For example, at 5°C, CCHFV can survive for up to 9 days on stainless steel surfaces and 8 days on plastic surfaces, thereby increasing the risk of indirect transmission via fomites.
| Phase | Incubation | Pre-hemorrhagic | Hemorrhagic | Convalescence |
|---|---|---|---|---|
| Timeline | 1–3 days after tick bite; 5–7 days (up to 13 days) after blood contact | Sudden onset, lasting 1–7 days | Begins 3–5 days after onset, lasts ~2–3 days | Begins 10–20 days after onset in survivors, may last up to 1 year |
| Key Clinical Features | Usually asymptomatic or mild thrombocytopenia |
|
|
|
The entry and pathogenic mechanisms of Crimean-Congo hemorrhagic fever virus (CCHFV) involve a complex, multifactorial process. During host cell entry, the virus relies on two parallel mechanisms: first, it utilizes host apolipoprotein E (ApoE) as a "molecular bridge," whereby the viral envelope protein Gc binds to cell surface low-density lipoprotein receptor (LDLR) to mediate endocytosis [4]; second, the soluble protein MFGE8 simultaneously binds to viral envelope phosphatidylserine (PtdSer) and cellular integrin receptors, enabling transmembrane entry [5]. Following successful entry into cells, the virus primarily targets mononuclear phagocytes, vascular endothelial cells, and hepatocytes. On one hand, it directly causes cytopathic effects and increases vascular permeability; on the other hand, it induces a vigorous and dysregulated "cytokine storm" (characterized by massive release of TNF-α, IL-6, and others), while suppressing the type I interferon response and delaying the production of specific antibodies. These pathological events ultimately lead to disseminated intravascular coagulation (DIC), shock, multi-organ failure, and death.
Laboratory diagnostic methods include detecting viral RNA in patient blood via PCR, or detecting viral antigens or specific antibodies (e.g., IgM) in serum using enzyme-linked immunosorbent assay (ELISA). Currently, there are no widely approved or highly effective specific antiviral therapies, and treatment remains primarily supportive.
CUSABIO closely monitors the latest developments in emerging virus research and provides high-quality recombinant proteins and ELISA kits to support viral detection, vaccine development, and studies on pathogenic mechanisms.
| Target | Product Name | Source | Tag Info | Code |
|---|---|---|---|---|
| N | Recombinant Crimean-Congo hemorrhagic fever virus Nucleoprotein (N) | E.coli | N-terminal 6xHis-B2M-tagged | CSB-EP328701CSB |
| GP | Recombinant Crimean-Congo hemorrhagic fever virus Envelopment polyprotein (GP), partial | E.coli | N-terminal MBP-tagged and C-terminal 6xHis-tagged | CSB-EP810349CSC1d8 |
| GP | Recombinant Crimean-Congo hemorrhagic fever virus Envelopment polyprotein (GP), partial-VLPs | Mammalian cell | C-terminal 10xHis-tagged (This tag can be tested only under denaturing conditions) | CSB-MP810349CSC |
| GP | Recombinant Crimean-Congo hemorrhagic fever virus Envelopment polyprotein (GP), partial | E.coli | C-terminal 6xHis-tagged | CSB-EP810349CSC2 |
| GP | Recombinant Crimean-Congo hemorrhagic fever virus Envelopment polyprotein (GP), partial (Active) | Mammalian cell | C-terminal 10xHis-tagged | CSB-MP810349CSC2 |
| Target | Product Name | Size | Sample Types | Code |
|---|---|---|---|---|
| EHF Ab (IgG) | Human anti-epidemic hemorrhagic fever virus antibody(IgG)ELISA Kit | 96T,5×96T,10×96T | serum | CSB-E09107h |
| EHF Ab (IgM) | Human anti-epidemic hemorrhagic fever virus(EHF) antibody(IgM) ELISA Kit | 96T,5×96T,10×96T | serum | CSB-E09553h |
| CSFV Ab (IgG) | Classical Swine Fever Virus Antibody(IgG) ELISA Kit | 96T,5×96T,10×96T | serum | CSB-E12765p |
Q:How can an ordinary person become infected with this virus?
The natural reservoirs of the virus are ticks of the genus Hyalomma, as well as domestic animals such as cattle, sheep, and camels. The most common route of infection is through the bite of an infected tick during outdoor activities. In addition, slaughtering infected animals, handling animal carcasses, or direct contact with the blood or secretions of infected patients also carries a very high risk of infection. Of note, the virus can survive for several days on surfaces such as stainless steel, increasing the potential for indirect contact transmission.
Q:What are the key receptors and molecular mechanisms underlying CCHFV entry into host cells?
CCHFV enters host cells primarily through two parallel pathways. The first utilizes host apolipoprotein E (ApoE) as a molecular bridge, whereby the viral envelope protein Gc binds to the low-density lipoprotein receptor (LDLR). The second involves the soluble protein MFGE8, which simultaneously binds to viral envelope phosphatidylserine (PtdSer) and cellular integrin receptors. These two mechanisms act synergistically to mediate viral endocytosis. The LDLR pathway is a recently discovered key entry route (Xu Z.S. et al., Cell Research, 2024), whereas the MFGE8 pathway represents a broad "phosphatidylserine bridging" mechanism. Understanding these molecular events provides direct targets for the development of receptor-blocking antiviral drugs.
Q:Are there any effective treatments available? What is immunotherapy?
Conventional treatment consists primarily of supportive measures, including fluid balance maintenance and correction of coagulation disorders. In recent years, progress has been made in immunotherapy: a neutralizing antibody named Gc13 can block viral entry into cells, while a non-neutralizing antibody (mAb-13G8) targeting the viral GP38 protein provides >90% protection when administered pre-exposure and >60% protection when administered post-exposure, making it a highly promising candidate therapy.
Q:What key factors are involved in the "cytokine storm" induced by CCHFV infection? Are there intervention strategies?
CCHFV infection induces massive release of cytokines such as TNF-α and IL-6. Anti-inflammatory treatments using TNF-α neutralizing antibodies or corticosteroids have shown partial protective effects in animal models. After the virus attacks mononuclear phagocytes and vascular endothelial cells, it triggers a vigorous and dysregulated immune response, manifested as disseminated intravascular coagulation (DIC), shock, and multi-organ failure. Studies have shown that post-exposure administration of TNF-α neutralizing antibodies provides partial protection, suggesting that anti-cytokine therapy is a promising avenue for exploration. This approach shares methodological parallels with the intervention logic used to manage cytokine release syndrome (CRS) in CAR-T therapy.
[1] Abdou Allayeh, et al. Stability of the Crimean-Congo Hemorrhagic Fever Virus on Inanimate Surfaces and Implications for Infection Control. Journal of Medical Virology. 2025; doi:10.1002/jmv.70575
[2] Ahata B, Akçapınar GB. CCHFV vaccine development, current challenges, limitations, and future directions. Frontiers in Immunology. 2023;14:1238882. doi:10.3389/fimmu.2023.1238882
[3] Frank MG, et al. Crimean Congo Hemorrhagic Fever Virus for Clinicians-Virology, Pathogenesis, and Pathology. Emerging Infectious Diseases. 2024;30(5). doi:10.3201/eid3005.231646
[4] McFadden E, et al. Engineering and structures of Crimean-Congo hemorrhagic fever virus glycoprotein complexes. Cell. 2025; doi:10.1016/j.cell.2024.11.008
[5] Xu ZS, et al. LDLR is an entry receptor for Crimean-Congo hemorrhagic fever virus. Cell Research. 2024; doi:10.1038/s41422-023-00917-w
Proteins
Antibodies
ELISA Kits