Call us
301-363-4651 (Available 9 a.m. to 5 p.m. CST from Monday to Friday)

Recently, the WHO has reported an outbreak of hantavirus infection on a polar expedition cruise ship that departed from Argentina on April 1. Starting from April 6, the virus has infected eight people, and as of May 7, three deaths have been recorded, raising public concern.
Hantaviruses belong to the Hantaviridae family within the order Bunyavirales. The virion structure of these viruses exhibits unique complexity, consisting of a lipid envelope, surface glycoprotein spikes, and an internal tripartite negative-sense RNA genome. These components work in concert to drive the entire viral life cycle, including host recognition, membrane fusion, and genome replication.
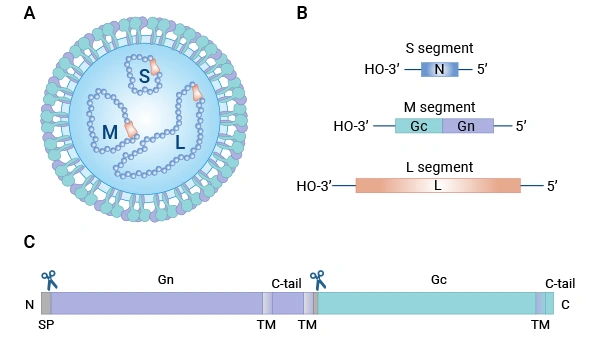
Figure 1. Schematic representation of hantavirus particle and genes.
Image source:PMID: 31439149
Research has found that there are over 20 types of hantaviruses that can cause distinct diseases, with significant differences in clinical manifestations depending on the virus species. They are primarily classified into hemorrhagic fever with renal syndrome and hantavirus pulmonary syndrome [1].
| Disease Type | Hemorrhagic fever with renal syndrome (HFRS) | Hantavirus Pulmonary Syndrome (HPS) |
| Main endemic regions | China, South Korea, Russia, Europe, etc. | The Americas (e. g., Argentina, the United States, etc.) |
| Major virus types | Hantaan virus, Seoul virus, etc. | Andes virus, Sin Nombre virus, etc. |
| Target organ | Kidney | Lung |
| Main clinical features | "Three Pains" (headache, lower back pain, orbital pain) + "Three Reds" (flushing of the face, neck, and chest) + bleeding + kidney damage。 | Fever, dry cough → respiratory distress, pulmonary edema, shock |
| Typical disease course | Febrile phase → Hypotensive shock phase → Oliguric phase → Polyuric phase → Convalescent phase | Sudden onset → rapid respiratory failure |
| Case fatality rate | Approximately 0.1% - 1% | Gundam 30% - 40% |
Hantavirus (represented by pathogenic types such as HTNV and ANDV) infection the core pathological event is Loss of vascular endothelial barrier integrity, leading to plasma extravasation, hemorrhage, and shock. The virus itself does not directly lyse endothelial cells, but rather through Immune-mediated injury Causeing dysfunction.
The virus enters the human body through inhalation of aerosols contaminated by the excreta of infected rodents, initially infecting alveolar macrophages and dendritic cells. Subsequently, the virus utilizes receptors such as β3 integrin (αVβ3) and DEC-205/DC-SIGN to enter vascular endothelial cells, macrophages, and renal tubular epithelial cells for efficient replication.
It is worth noting that the virus exhibits a "latent infection" characteristic in endothelial cells without directly causing cytopathic effects. After endothelial cells are infected with hantavirus, they secrete vascular endothelial growth factor (VEGF), which triggers the downregulation of VE-cadherin in adherens junctions, thereby disrupting tight junctions between endothelial cells and leading to increased vascular permeability. At the same time, infected endothelial cells also produce pro-inflammatory cytokines and chemokines, such as IP-10 and RANTES, and upregulate cell surface adhesion molecules. As the viral load increases, the host's immune system becomes overactivated. Recruited monocytes and macrophages polarize into a pro-inflammatory M1 phenotype, releasing large amounts of inflammatory cytokines such as TNF-α, IL-6, and CXCL10, thus forming a "cytokine storm." In addition, CD8+ T cells cause secondary damage to the endothelial barrier during the clearance of virus-infected endothelial cells, ultimately leading to severe clinical consequences such as significantly increased vascular permeability, plasma extravasation, shock, kidney injury, and hemorrhage [2].
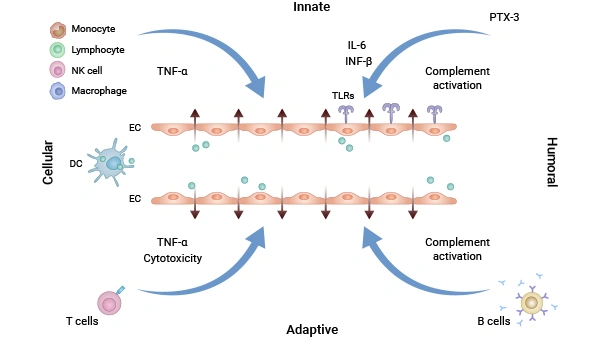
Figure 2. Both humoral and cellular components of the innate and adaptive immune systems can contribute to vascular leakage. In response to hantavirus-infected endothelial cells (ECs), neutrophils release inflammatory cytokines such as TNF-α, which directly or indirectly enhance vascular permeability.
Image source:PMID 35384417
This pathological process is not driven by direct viral lysis of cells but rather results from a dysregulated host immune response, which also provides a critical intervention point for targeted immunomodulation—such as restoring interferon signaling, inhibiting RIPK3, or mimicking the natural host's inflammatory self-limiting mechanisms.
For more details, please click: What You Have to Know about Cytokine Storm and Virus Infection
In hantavirus infection, this immune system "storm" is not driven by a single factor but results from the combined action of multiple key molecules and signaling pathways, exacerbating fatal outcomes such as vascular leakage and multi-organ failure. The essence of a cytokine storm is the excessive production of pro-inflammatory factors. The core cytokines involved in the viral immune response fall into the following main categories:
CUSABIO provides the following professional tools to support research in viral immunology and related therapies:
| Target | Product Name | Size | Sample Types | Code |
|---|---|---|---|---|
| IgG | Human hantavirus (HV) antibody (IgG) ELISA kit | 96T,5×96T,10×96T | serum | CSB-EQ028036HU |
| IgM | Human hantavirus (HV) antibody (IgM) ELISA kit | 96T,5×96T,10×96T | serum | CSB-EQ027544HU |
| Target | Product Name | Source | Tag Info | Code |
|---|---|---|---|---|
| GP | Recombinant Hantaan virus Envelopment polyprotein (GP), partial | Baculovirus | C-terminal 6xHis-tagged | CSB-BP357454HCB1 |
| GP | Recombinant Hantaan virus Envelopment polyprotein (GP), partial | Mammalian cell | C-terminal 6xHis-tagged | CSB-MP357454HCB1 |
| N/A | Recombinant Orthohantavirus hantanense Envelopment polyprotein, partial | Yeast | C-terminal 6xHis-tagged | CSB-YP4799GTQ |
| N/A | Recombinant Orthohantavirus hantanense Envelopment polyprotein, partial | Mammalian cell | C-terminal hFc1-tagged | CSB-MP4799GTQ |
| N | Recombinant Hantaan virus Nucleoprotein (N) | E.coli | N-terminal 6xHis-tagged | CSB-EP361470HCB |
The main transmission routes of hantavirus involve rodents and include the following three modes:
Inhalation of aerosols generated from urine, feces, or saliva of infected rodents.
Ingestion of food or water contaminated with excreta from infected rodents.
Being bitten or scratched by infected rodents, or direct/indirect contact of broken skin or mucous membranes with rodent excreta or contaminated materials.
Hantavirus infection generally does not spread from person to person, and routine social interactions or public contact do not pose a risk of transmission.
Hantavirus infections exhibit a wide geographical distribution globally, with an estimated 200,000 infection cases worldwide each year. Its epidemiological characteristics are influenced by various factors, including climate, environment, social development, the ecology of rodent hosts, and human behavior [4]. In the Americas, Sin Nombre virus (SNV) is the primary pathogen causing hantavirus cardiopulmonary syndrome (HCPS). As of January 2020, 143 laboratory-confirmed cases have been identified in Canada alone.
In China, the main hosts include the striped field mouse (Apodemus agrarius) and the brown rat (Rattus norvegicus). A spatiotemporal predictive analysis of data from China between 2005 and 2028 indicates that viruses carried by the brown rat (Rattus) will be the most active in terms of transmission in the future, with risks even surpassing those in regions dominated by the striped field mouse (Apodemus) [5]. In Europe, such as in Poland, hantavirus infections are primarily caused by the Puumala and Dobrava serotypes. In Russia, over 130,000 cases of HFRS have been reported in the past 20 years, with 98.4% occurring in western Russia. Differences in serotypes have led to significant variations in mortality rates.
The clinical manifestations of HFRS are diverse, typically including fever, myalgia, headache, lower back pain, and gastrointestinal symptoms.Since viremia appears in the early stages of the disease and can persist for more than two weeks, viral load has become an important indicator for early diagnosis. Studies have found that viral load is positively correlated with white blood cell, lymphocyte, and monocyte counts, but negatively correlated with platelet count [6].
In addition to directly detecting the virus,Thrombomodulin (TM), Plasma BNP level, Procalcitonin (PCT), Osteoprotegerin (OPG) Multiple biomarkers have been confirmed.It has significant predictive value for assessing the severity of the disease. In addition, leukocytosis, thrombocytopenia, proteinuria, hematuria, coagulation abnormalities, and electrolyte disturbances (such as hyponatremia and hypocalcemia) are also common laboratory features in patients with HFRS, including children. For adult patients, hypotensive shock, myoglobin levels, and neutrophil counts have also been identified as independent factors for predicting the risk of critical illness. Currently, there is still a lack of specific etiological therapy for hantavirus infection. Animal model studies have provided directions for treatment: a targetedHantavirusThe neutralizing monoclonal antibody HCO2 against the virus, when administered on the fifth day post-infection, can also alleviate weight loss and renal medullary hemorrhage in mice, though earlier administration yields better results. This suggests that the timing of immunotherapy is crucial.
CUSABIO focuses on key nodes in the immunopathology of hantavirus infection. We are committed to simulating the natural host's inflammatory self-limiting mechanism to block the "cytokine storm" at its root, providing full-chain support for Hemorrhagic Fever with Renal Syndrome (HFRS) and Hantavirus Pulmonary Syndrome (HPS), from biomarker discovery to early development of antibody drugs.
Q:Why does hantavirus infection cause severe vascular leakage and even shock?
Vascular leakage caused by hantavirus infection is primarily due to uncontrolled host immune responses rather than direct viral destruction of cells. The virus does not directly lyse endothelial cells; instead, it activates the immune system after infection, inducing a cytokine storm, recruiting inflammatory cells, and disrupting the connections between vascular endothelial cells, ultimately leading to plasma extravasation, decreased blood pressure, and shock.
Q:Why do the types and severity of diseases caused by different hantaviruses vary significantly?
Different virus types exhibit varying preferences for target organs, leading to two distinct clinical manifestations: hemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome (HPS). There are over 20 pathogenic types of hantavirus. For instance, the Hantaan virus primarily attacks the kidneys, causing HFRS, while the Andes virus mainly targets the lungs, resulting in HPS. The two differ significantly in disease progression, symptom characteristics, and case fatality rates (approximately 0.1–1% for HFRS vs. 30–40% for HPS).
Q:Is there a specific therapeutic drug for hantavirus at present?
Currently, there is no specific antiviral therapy, and immunomodulation along with early neutralizing antibody intervention are important treatment directions. Clinical management remains primarily supportive; however, in animal models, administration of neutralizing monoclonal antibodies (such as HCO2) during the early stages of infection can reduce renal hemorrhage and weight loss, suggesting that targeting immune responses or antibody therapy holds potential value.
Q:How to accurately diagnose hantavirus infection at an early stage?
Early diagnosis primarily relies on viral load testing, combined with the assessment of multiple blood and urine biomarkers to evaluate disease severity. In the early stages of onset, viremia can persist for more than two weeks. Viral load is positively correlated with white blood cell and lymphocyte counts and negatively correlated with platelet count. Meanwhile, markers such as thrombomodulin, procalcitonin, and osteoprotegerin can be used to assess the risk of disease severity.
Q:What key tools can CUSABIO provide for hantavirus research?
CUSABIO provides a comprehensive range of research tools, including ELISA detection kits for key cytokines such as TNF-α, IL-6, IL-18, and RANTES; recombinant proteins for hantavirus GP and N proteins (suitable for vaccine and immune mechanism research); and a full series of anti-payload antibodies required for ADC drug development.
[1] Tkachenko E, et al. Clinical Manifestations of Hemorrhagic Fever with Renal Syndrome, Various Nosologic Forms and Issues of Hantavirus Infections Terminology. Viruses. 2025;17(4):578. doi:10.3390/v17040578
[2] Su L, et al. Dynamic alterations of circulating lymphocytes during the trajectory of Hantaan virus-induced hemorrhagic fever with renal syndrome. Front Immunol. 2025;16:1354892. doi:10.3389/fimmu.2025.1354892
[3] Garanina E, et al. Cytokine Storm Combined with Humoral Immune Response Defect in Fatal Hemorrhagic Fever with Renal Syndrome Case, Tatarstan, Russia. Viruses. 2019;11(7):601. doi:10.3390/v11070601
[4] Vial PA, et al. Hantavirus in humans: a review of clinical aspects and management. Lancet Infect Dis. 2023;23(9):e371-e382. doi:10.1016/S1473-3099(23)00128-7
[5] Wang Y, et al. Spatiotemporal trends of hemorrhagic fever with renal syndrome (HFRS) in China under climate variation. Proc Natl Acad Sci USA. 2024;121(4):e2312556121. doi:10.1073/pnas.2312556121
[6] Ma S, et al. Temporal Dynamics of Viremia in Hemorrhagic Fever With Renal Syndrome Patients. J Med Virol. 2026;98(5):e70963. doi:10.1002/jmv.70963
Proteins
Antibodies
ELISA Kits